Best Birth Control for Perimenopause: A 2026 Guide
Find the best birth control for perimenopause. Our 2026 guide compares hormonal and non-hormonal options for symptom relief, weight, and safety.
If you're in your 40s or early 50s and suddenly your period has become unpredictable, your sleep is worse, your waist feels less forgiving, and your old birth control no longer feels like a simple routine, you're not imagining it. Perimenopause changes the job birth control has to do.
At this stage, contraception isn't only about preventing pregnancy. It may also need to help with heavy bleeding, erratic cycles, hot flashes, mood shifts, bloating, and the frustrating question many women ask in clinic: “Is this method helping me, or making me feel worse?”
The best birth control for perimenopause depends less on a single “best” product and more on your symptom pattern, your cardiovascular risk, your tolerance for hormones, and what matters most to you day to day. For some women, a low-dose combined pill is the most useful tool. For others, a hormonal IUD is the safer and smarter choice. And for women who are especially focused on weight changes, metabolic health, or staying off hormones, non-hormonal options deserve more attention than they usually get.
Why Perimenopause Changes Your Contraception Needs
Perimenopause is a hormonally uneven phase. You may still ovulate, but not predictably. That means pregnancy is still possible even when your cycle looks chaotic. At the same time, estrogen and progesterone shifts can drive symptoms that younger women on birth control often aren't dealing with yet.
What changes in practice is this: the “right” method has to do more than provide contraception. It often has to control bleeding, smooth out hormonal swings, or avoid making certain symptoms worse.
The new goal is dual-purpose treatment
Earlier in life, women often chose contraception based on convenience, side effects, or reliability alone. In perimenopause, I usually see a second agenda appear. A patient wants contraception, yes, but she also wants less flooding, fewer surprise periods, fewer nighttime symptoms, and less disruption at work or while traveling.
That changes the discussion.
Some methods suppress cycle instability well. Some protect against pregnancy but do little for hot flashes or mood volatility. Some reduce bleeding dramatically but may cause spotting at first. Some avoid estrogen, which is important if you have migraine with aura, high blood pressure, a history of blood clots, or other contraindications.
Weight and bloating deserve a real conversation
This is one of the biggest gaps in routine counseling. Many women don't only want to know whether a method stops pregnancy. They want to know whether they'll feel swollen, hungrier, flatter emotionally, or less like themselves.
A Women's Health Network review of birth control in perimenopause notes that metabolic health is an underserved angle and cites 2025 data showing average weight gain of +2.5 kg over 2 years with combined oral contraceptives versus +1.1 kg with progestin-IUDs in perimenopause, with many unanswered patient questions focused on weight gain and bloating.
The best birth control for perimenopause isn't automatically the one that helps hot flashes most. It's the one that addresses your symptoms without creating a second set of problems you hate living with.
A quick comparison of the main options
Method | Good fit for | Main strengths | Main trade-offs |
|---|---|---|---|
Low-dose combined pill | Women who want cycle control plus symptom relief and can safely use estrogen | Predictable bleeding, contraception, may ease perimenopausal fluctuations | Not appropriate for some women with estrogen-related risks |
Patch or vaginal ring | Women who want combined hormones without a daily pill | Steady delivery, less daily hassle | Same estrogen-related safety limits |
Hormonal IUD | Women with heavy bleeding or who need to avoid estrogen | Strong bleeding control, long-acting contraception | Irregular bleeding can happen early on, less help for whole-body symptoms |
Progestin-only pill, implant, or shot | Women who can't use estrogen | Estrogen-free contraception | Bleeding patterns can be unpredictable |
Copper IUD or barrier methods | Women who want non-hormonal contraception | No hormone exposure, preserves natural cycle patterns | Doesn't treat perimenopausal symptoms |
Why standard birth control advice stops working
General birth control advice often assumes a younger woman with stable ovarian function. Perimenopause isn't that. Symptoms become part of the treatment decision, and so do long-term questions about when to stop contraception and when to consider menopause-focused hormone therapy.
That is why a method that was “fine for years” can suddenly feel wrong. Your body changed. Your goals changed. Your birth control may need to change too.
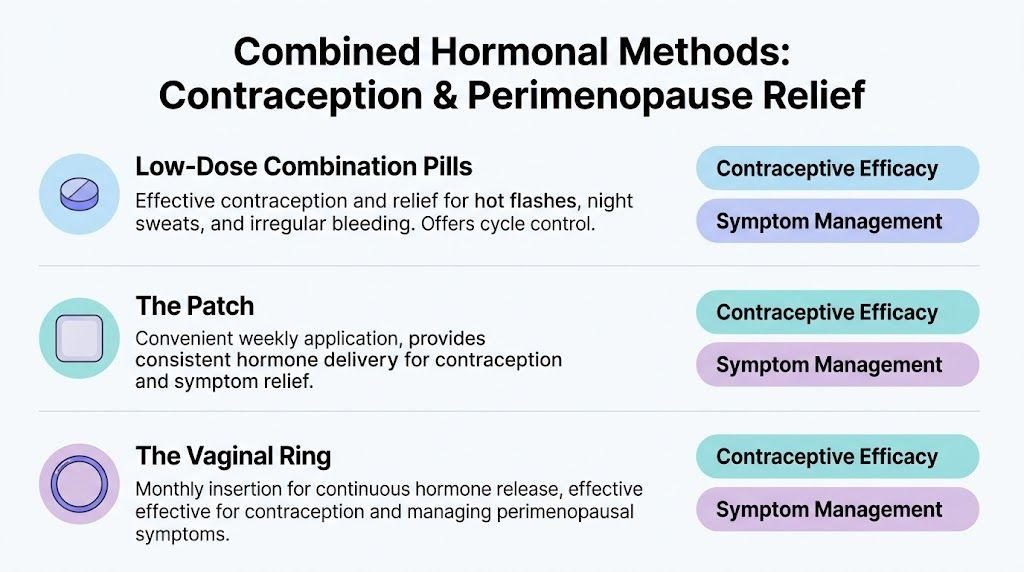
Combined Hormonal Methods for Contraception and Symptom Relief
For many healthy perimenopausal women, combined hormonal contraception remains the most useful option because it can do two jobs at once. It prevents pregnancy and reduces hormone fluctuation enough to make daily life more predictable.
This category includes combined oral contraceptive pills, the patch, and the vaginal ring. All contain estrogen plus progestin. The differences are mostly about delivery, convenience, and how well each fits your routine.
Low-dose combination pills
Combined pills are the most familiar choice, and in perimenopause they often work well when the goal is to regulate chaos. A review on combined oral contraceptive use in perimenopausal women found that COCs reduce menstrual bleeding by approximately 40%, and that estradiol valerate/dienogest formulations reduce bleeding by more than 50% in 70% of users. The same review notes a failure rate of less than 1% for pregnancy prevention and describes 20 micrograms of ethinyl estradiol as standard in low-dose practice, with Loestrin 1/20 and Loestrin 24 commonly prescribed.
That matters because the best birth control for perimenopause often needs to control heavy bleeding without exposing you to more hormone than necessary.
Clinical sweet spot: A low-dose combined pill is often the first method I think about when a patient wants better cycle control, lighter periods, and reliable contraception in one prescription.
Combined pills may also offer broader benefits during this phase. The same review notes reduced risk of ovarian, endometrial, and colorectal cancers, along with protection from bone loss during the perimenopausal transition.
Why some women do better on pills than on other combined methods
Pills give you the most formulation options. That's useful if you're trying to adjust the estrogen dose or choose a progestin with fewer androgen-related side effects. If bloating, libido changes, or mood flattening become an issue, changing pill formulation is often easier than changing categories entirely.
They also offer flexibility. Some women do better with a traditional cycle. Others feel much better taking active pills continuously to avoid hormone-withdrawal bleeding and monthly symptom flare.
The patch
The patch delivers combined hormones through the skin. Its practical advantage is obvious. You don't need to remember a pill every day.
For women who are good candidates for estrogen, the patch can be a strong option when adherence is the biggest issue. If daily pills are getting missed because of travel, ADHD, caregiving overload, or simple fatigue with routines, a weekly method can improve consistency.
The trade-off is that it still carries the same estrogen-related eligibility concerns as combined pills. If estrogen is not safe for you, the patch isn't the workaround.
If your symptoms improve on combined hormones but you struggle to take a pill on schedule, changing the delivery system often works better than abandoning the hormone class.
The vaginal ring
The ring gives monthly rather than daily management and offers steady hormone release. Many women like it because it feels low-maintenance without committing to a longer-acting device.
In practice, the ring often suits women who want cycle control and symptom smoothing but don't want to think about contraception every day or every week. Some women also find the ring easier on the stomach than pills, because it bypasses the routine of oral dosing, though individual experience varies.
Who should not use combined hormonal methods
This is the point where safety matters more than convenience. Combined hormonal contraception is not the best birth control for perimenopause if you have clear contraindications to estrogen.
Women who smoke and are over 35, have a history of blood clots or cardiovascular disease, develop severe headaches with estrogen, have high blood pressure, or take certain interacting medications need a different path. Those situations push the decision toward progestin-only or non-hormonal options.
Pills, patch, or ring
A simple way to think about the choice is this:
Choose pills if you want the most formulation flexibility and the easiest path for dose adjustment.
Choose the patch if your biggest problem is remembering a daily method.
Choose the ring if you want a low-maintenance combined option without a weekly task.
For women who are beginning to think ahead to menopause treatment, it also helps to understand that birth control and menopause hormone therapy aren't the same thing. If you want a primer on that distinction, this guide to hormone therapy for menopause is a useful next read.
Progestin-Only and Non-Hormonal Contraceptives
If estrogen isn't safe for you, or you don't want it, the conversation shifts. This group includes hormonal IUDs, progestin-only pills, the implant, the shot, and non-hormonal choices such as the copper IUD and barrier methods.
These methods can be excellent, but they solve different problems than combined methods do. The key is matching the method to the symptom pattern you have.
Hormonal IUDs for heavy bleeding
For many perimenopausal women, the levonorgestrel IUD is the standout option when bleeding is the main issue. A clinical review of contraception during perimenopause describes the levonorgestrel-releasing intrauterine system as the most effective method against abnormal uterine bleeding, and notes that hormonal IUDs provide 3 to 7 years of pregnancy protection. The same review explains that approximately 50% of women using certain contraceptives experience alterations in bleeding patterns and highlights that many hormonal IUD users eventually have much lighter periods or no bleeding at all.
That local uterine effect is the reason many women love it. It can dramatically reduce the burden of heavy, drawn-out, unpredictable bleeding without exposing the whole body to estrogen.
When a hormonal IUD is often the best choice
A hormonal IUD is especially attractive if this sounds like you:
Heavy bleeding is your main problem. If you're soaking through products, planning your life around bathrooms, or feeling wrung out by long periods, this option deserves serious discussion.
You need to avoid estrogen. This includes women with blood clot history, high blood pressure, smoking over age 35, certain medication interactions, or estrogen-triggered headaches.
You want a set-it-and-forget-it method. Once placed, it doesn't require daily action.
One limitation is important. A hormonal IUD can be excellent for bleeding control and contraception, but it won't usually provide the same whole-body symptom relief that some women get from combined methods. If hot flashes, night sweats, or mood swings are your dominant problem, a hormonal IUD may not be enough on its own.
Progestin-only pills, implant, and shot
These methods matter because they fill the estrogen-free gap, but they tend to be less elegant for cycle control.
The mini-pill can work well for pregnancy prevention, but bleeding irregularity is common. The implant is convenient and long-acting, but some women stop it because the bleeding pattern becomes too unpredictable. The shot can be useful in select cases, though many perimenopausal women want something more reversible or easier to fine-tune.
In clinic, these methods are often best when safety is the overriding priority and the patient understands that bleeding may be less predictable than with combined pills or a hormonal IUD.
The method that is safest for you may not be the one that gives the neatest cycle. That's frustrating, but it's an honest trade-off worth discussing upfront.
Copper IUD and barrier methods
The copper IUD doesn't contain hormones. That's its biggest selling point in perimenopause.
For women who are highly sensitive to hormonal side effects, who want to observe their natural cycle patterns more clearly, or who are focused on avoiding any possible hormone-related effect on bloating or metabolic tracking, the copper IUD can be a very reasonable option. Its drawback is equally straightforward. It prevents pregnancy, but it does not treat perimenopausal symptoms and may not be ideal if your periods are already heavy.
Barrier methods such as condoms can also work well, particularly for women with declining fertility who prioritize hormone-free contraception and don't need cycle control. They ask more of you in real life, though. You have to use them correctly every time, and they don't help with bleeding, sleep disruption, or vasomotor symptoms.
What tends not to work well
The biggest mismatch I see is choosing a method for its contraceptive reliability while ignoring the symptom profile.
Examples:
A woman with very heavy bleeding choosing a copper IUD first. The method may be effective for contraception but disappointing for symptom burden.
A woman with estrogen contraindications pushing to stay on a combined pill. Symptom relief isn't worth compromising safety.
A woman whose main complaint is hot flashes expecting a progestin-only method to fix everything. It may protect against pregnancy but leave the core issue untouched.
The best birth control for perimenopause often comes down to accepting that each option has a shape. Some are broad symptom managers. Some are targeted tools. Some are mainly contraceptives.
Choosing the Best Birth Control for Your Unique Symptoms
Most women don't need more birth control categories. They need a practical way to narrow the list.
Start with the symptom or concern that bothers you most. Not the one you think should matter most. The one that is disrupting your life.
If your main issue is very heavy or prolonged bleeding
Think first about a hormonal IUD. It is usually the strongest targeted choice when the uterus is the center of the problem.
A low-dose combined pill can also be a good fit if you're medically eligible for estrogen and want both contraception and broader symptom control. Between the two, I usually favor the IUD when bleeding is the dominant complaint and convenience matters. I lean toward the pill when the woman also wants help with cyclic symptoms that extend beyond the uterus.
If your biggest concern is weight, bloating, or feeling hormonally “off”
Many women often feel dismissed. They know when a method changes appetite, fluid retention, breast tenderness, or how their clothes fit, even when that effect doesn't show up neatly in a brief office visit.
In that situation, a copper IUD or careful consideration of a hormonal IUD may make more sense than defaulting to a combined pill. If you do use systemic hormones, ask directly about trying the lowest effective dose and whether a different formulation could reduce unwanted side effects.
A symptom-based record can also help. Women dealing with vaginal dryness, irritation, urinary urgency, or discomfort with intimacy may also be dealing with a separate menopause-related issue, and this overview of genitourinary syndrome of menopause can help you tell those symptoms apart from birth-control side effects.
If you need to avoid estrogen
This is a straightforward branch point. If you have migraine with aura, high blood pressure, a history of blood clots, smoking over 35, or another estrogen contraindication, skip combined pills, the patch, and the ring.
The most useful options to discuss are:
Hormonal IUD if bleeding is heavy
Progestin-only pill if you want a pill format
Implant or shot if you prefer a longer-acting estrogen-free method
Copper IUD if you want no hormones at all
That doesn't automatically mean one of these will feel perfect. It means they're the safer menu.
If convenience matters more than anything
Some women don't want another daily task. That's valid.
The methods that usually fit best are:
Hormonal IUD for long-term contraception plus bleeding benefit
Copper IUD for long-term contraception without hormones
Patch if you want combined hormones but not a daily pill
Ring if monthly management sounds easiest
This video gives a helpful visual overview before you take your shortlist to a clinician.
▶ PlayA simple decision filter
When you're trying to identify the best birth control for perimenopause, bring it back to four questions:
What symptom am I most trying to change
Is estrogen safe for me
Do I want local treatment or whole-body symptom support
How much maintenance am I realistically willing to do
Pick the method that matches your real life, not the one that sounds ideal on paper. A great option you won't use consistently is not a great option for you.
Planning Your Transition from Contraception to Menopause
This is one of the most confusing parts of the whole process. Many women assume that irregular periods mean fertility is basically over, or that staying on the pill too long is wrong. Neither assumption is reliable.
A guide on birth control during perimenopause notes that contraception is advised until age 50 to 55, and that there is major uncertainty around switching from the pill to menopause treatment. The same source describes concern about long-term use, bone density, and breast cancer risk, including an OR of 1.24 for combined pills used more than 5 years.
Why the transition is so unclear
Hormonal contraception can mask the very signs women use to judge menopause. If you're on the pill and not bleeding, that doesn't necessarily mean you've reached menopause. It may mean the medication is controlling the cycle.
That is why women often feel stuck. They don't know whether to continue contraception, taper off, or switch to a menopause-focused regimen.
A practical way to think about the switch
Contraceptive hormones and menopause hormones aren't interchangeable. Birth control is designed to suppress ovulation and prevent pregnancy. Menopause therapy is designed to treat symptoms using a different hormonal strategy.
A careful transition plan usually includes these points:
Review whether pregnancy prevention is still needed. Age matters, but so does whether you're still potentially ovulating.
Reassess symptom goals. If your main issue has become hot flashes, sleep disruption, or vaginal symptoms rather than contraception, a different treatment model may fit better.
Plan the switch with a clinician. This is not the moment for guesswork, especially if you've had bleeding changes, migraine history, clot risk, or breast concerns.
If you want a broader clinical overview of Hormone Replacement Therapy (HRT), a physician-led explanation can help clarify how HRT differs from birth control after menopause is confirmed or strongly suspected.
Testing and timing questions
One of the hardest parts is that testing isn't always simple or decisive while you're using hormonal contraception. If you're trying to understand what testing can and can't tell you, this article on testing for perimenopause is a helpful place to start.
Planning point: Don't wait until you're miserable on a method to ask about the exit plan. If you're in your late perimenopausal years, ask your clinician now how they decide when to stop contraception and when to consider HRT.
Partnering with Your Doctor on Your Perimenopause Plan
The best birth control for perimenopause is a medical decision, but it should also be a collaborative one. Your clinician brings safety screening and prescribing expertise. You bring the symptom history, preferences, and lived reality.
Appointments go better when you arrive with specifics. “I feel off” is true, but “my bleeding lasts longer, I wake up hot, and I gained weight on my last pill” gives your clinician something usable.
Bring these questions to your visit:
Safety first: “Is estrogen safe for me based on my blood pressure, migraine history, smoking status, and medication list?”
Symptom priority: “Which option is most likely to help my main problem, bleeding, hot flashes, bloating, or convenience?”
Bleeding expectations: “What bleeding pattern should I expect in the first few months, and when should I call if it doesn't settle?”
Metabolic concerns: “If I already struggle with weight gain or bloating, which methods are least likely to make that harder for me?”
Transition planning: “How will we know when it's time to stop contraception and consider menopause treatment instead?”
Good care isn't about being handed one option. It's about reviewing trade-offs thoroughly and choosing the method that fits both your medical profile and your life.
Frequently Asked Questions About Perimenopause Contraception
Can HRT replace birth control during perimenopause
Usually, no. Menopause hormone therapy is not designed to prevent pregnancy. If you are still in perimenopause and pregnancy is possible, you generally still need contraception unless your clinician confirms otherwise.
Can I take birth control continuously to skip periods
For many women, yes, continuous use of combined hormonal contraception is a practical strategy. It can reduce withdrawal bleeding and monthly symptom flares. Whether it's appropriate depends on the method and your medical history.
How do I know if I've reached menopause while on the pill
This can be difficult because hormonal contraception may mask your natural cycle. Lack of bleeding on the pill doesn't prove menopause. That question usually requires an individualized plan with your clinician.
Is the hormonal IUD enough if I also have hot flashes
Not always. A hormonal IUD is often excellent for heavy bleeding and contraception, but it may not address whole-body symptoms the way combined methods can. Some women need separate treatment for those symptoms.
What if I hate how I feel on hormones
That matters. Side effects that affect mood, bloating, libido, or weight tolerance are part of the decision, not a minor footnote. If you feel worse on a method, tell your clinician plainly. There are other options.
If you want help making sense of symptoms day to day, Lila offers AI-guided tracking for cycles, sleep, mood, energy, bloating, and hot flashes so you can spot patterns, see what’s changing, and walk into your next appointment with clearer data about what your body is doing.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.