Can You Test For Perimenopause? Expert Answers.
Can you test for perimenopause - Can you test for perimenopause? Learn why hormone tests are often unreliable and discover the clinical methods and tracking too

You wake up at 3 a.m. again. Your period came early last month, then disappeared this month. You feel more anxious than usual, your patience is thinner, and your body doesn’t quite feel like your own. So you do what almost everyone does. You search: can you test for perimenopause?
It’s a very reasonable question.
Most of us are taught to expect a clean medical answer. Strep test. Pregnancy test. Cholesterol test. You want one clear result that says yes, this is perimenopause, or no, it’s something else. When your symptoms are affecting sleep, work, relationships, and confidence, that kind of certainty sounds like relief.
The frustrating part is that perimenopause usually doesn’t work that way. The answer isn’t a neat yes-or-no lab result. But that doesn’t mean you’re stuck guessing, and it doesn’t mean your symptoms aren’t real.
The Search for a Simple Answer to Perimenopause
You notice your period is suddenly unpredictable. Then the sleep problems start. Then come the days when you feel edgy, foggy, or unlike yourself, and it becomes hard to tell whether you are dealing with stress, a thyroid issue, depression, burnout, or the hormonal transition you have heard about but never fully understood.
That uncertainty can wear you down fast.
Perimenopause is the transition leading up to menopause, and it often begins earlier than expected. Menopause itself is defined as 12 straight months without a period, and the National Institute on Aging explains that the average age is 52. The years before that point are often uneven. Symptoms can come and go, periods may still happen, and the pattern rarely looks neat while you are living through it.
Why this feels so confusing
Perimenopause does not follow a tidy script.
One person notices cycle changes first. Another notices anxiety, poor sleep, hot flashes, low mood, or brain fog long before periods become clearly irregular. You can still be having periods and still be in perimenopause. That point trips people up because we are taught to associate menopause with periods stopping, when the transition usually starts well before that final milestone.
A helpful way to frame it is this. Menopause is the finish line. Perimenopause is the long, winding stretch of road before it.
You do not have to reach menopause for hormone-related changes to affect your daily life.
The question behind the question
When you ask whether you can test for perimenopause, you are usually asking for something deeper than a lab value.
You want a clear answer. You want your experience to make sense. You want to know that the mix of symptoms is connected, not random.
That desire makes complete sense. We are used to health questions having a simple test and a simple result.
Perimenopause rarely gives us that kind of clean yes-or-no answer. A single hormone result is often like one photo of a rough ocean. It captures one real moment, but not the full pattern. What helps more is tracking the pattern over time, especially your symptoms and cycle changes. That is why tools built for symptom tracking, including apps like Lila, can be more useful than one isolated test result.
Why a Single Hormone Test Usually Fails
A single hormone test fails for the same reason a single photo can’t explain a turbulent ocean.
If you stand on the shore during a storm and snap one picture of one wave, you’ve captured a real moment. But you haven’t captured the tide, the current, or the pattern of the sea. Hormones in perimenopause work in a similar way. One reading can be real and still be misleading.
A test result is a snapshot, not the whole story
Single-point blood, urine, or saliva tests provide only a snapshot. They can’t reliably tell you whether you’re in perimenopause because hormones such as FSH naturally rise and fall across the cycle, and higher FSH levels can occur both before ovulation and during the perimenopausal transition, as explained in this Mayo Clinic video discussion on perimenopause testing.
That’s why many women get a “normal” result even when their symptoms are very real.
On another day, that same woman might get a completely different number.
Perimenopause is not a smooth decline
Many people picture perimenopause as a straight line downward. That would be much easier to test.
In reality, hormone patterns often behave more like a roller coaster. Levels can swing up and down from one day to the next, and sometimes even more quickly than that. That means a lab result can tell you what happened at that moment, but not whether the broader pattern fits perimenopause.
If you’ve ever looked up normal estradiol levels, confusion often starts at this point. A result might fall inside a reference range and still not settle the question, because perimenopause is defined less by one isolated number and more by changing patterns over time.
Why this leads to mixed messages
A woman can have symptoms that strongly fit perimenopause and still hear that her hormones are “fine.”
That doesn’t always mean the clinician is dismissing her. Sometimes the test isn’t capable of answering the question she hoped it would answer.
Practical rule: If a hormone level changes unpredictably, one lab draw can confirm very little on its own.
This is also why testing can feel emotionally rough. You feel unwell, you do the responsible thing, and the result seems to say nothing useful. The problem isn’t that you imagined the symptoms. The problem is that the tool was limited.
Understanding the Different Hormone Tests Available
Doctors may still order tests in certain situations. The key is knowing what each test can and cannot tell you.
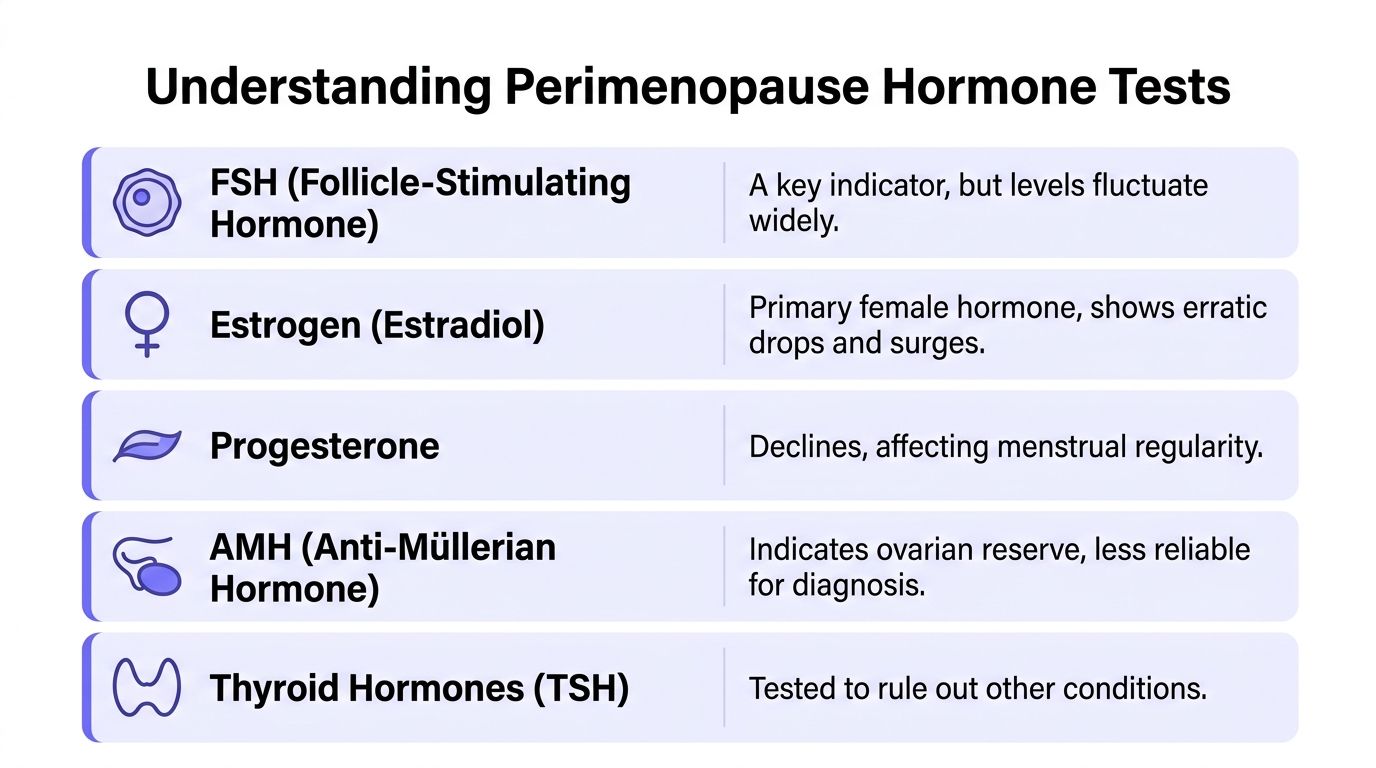
FSH and estradiol
FSH, or follicle-stimulating hormone, often gets the most attention. It reflects how hard the brain is signaling the ovaries. In later reproductive transition, FSH may trend higher. The problem is that it doesn’t stay put.
A higher FSH level can appear during normal cycle variation as well as during perimenopause. That’s why it can hint at change without giving a dependable answer by itself.
Estradiol is a form of estrogen. Many women expect it to steadily drop during perimenopause, but that’s not how the body usually behaves. Estradiol can surge and dip in irregular ways. A single result may look reassuring one day and confusing the next.
AMH and what it means
AMH, or anti-Müllerian hormone, is different. It’s a more technically precise marker of ovarian reserve. According to a review on ovarian aging and biomarkers, AMH below 0.2 ng/mL can indicate imminent menopause, but it is not a standalone diagnostic tool for perimenopause and should be interpreted alongside other clinical information and thyroid testing in appropriate cases, as described in this PMC review of biomarkers including AMH.
That sounds promising, but the limitation matters.
AMH says more about ovarian reserve than about your day-to-day stage in the transition. It may be useful in a broader evaluation, especially in more complex cases, but it doesn’t replace the clinical picture.
Thyroid testing matters more than many women realize
Thyroid problems can look a lot like perimenopause.
Fatigue, brain fog, weight changes, mood shifts, and feeling unlike yourself can all happen with thyroid dysfunction. That’s why thyroid testing often plays a more practical role than people expect when symptoms are confusing.
If you’re sorting through whether symptoms fit hormonal transition or another condition, this guide on testing for menopause can help frame what tests are useful versus what sounds useful.
A quick comparison
Hormone | What It Measures | Usefulness in Perimenopause Diagnosis |
|---|---|---|
FSH | Pituitary signaling to the ovaries | May support the picture, but fluctuates too much to diagnose on its own |
Estradiol | A key estrogen level at one point in time | Often erratic in perimenopause, so one result can mislead |
AMH | Ovarian reserve | More stable than FSH, but not a standalone perimenopause test |
Thyroid hormones | Thyroid function | Useful for ruling out conditions that mimic perimenopause |
Progesterone | Ovulation-related hormone patterns | Can reflect changing ovulation, but isn’t a simple diagnostic answer |
When tests can still help
Testing isn’t useless. It’s just easy to overestimate what it can do.
A clinician may order labs to:
Rule out another condition. Thyroid disease is a common example.
Investigate symptoms under age 40. In that setting, clinicians may want to screen for primary ovarian insufficiency, which is a different diagnosis.
Clarify a complicated picture. This matters when the symptom pattern doesn’t fit neatly, or when treatment planning calls for a broader workup.
A good lab panel can answer the question “Could this be something else?” even when it can’t answer “Is this definitely perimenopause?”
How Doctors Diagnose Perimenopause
You go to your appointment hoping for a clean answer. Maybe one blood test, one number, one clear label. Instead, your doctor starts asking about your periods, your sleep, your mood, and whether your body feels different than it did a year ago.
That can sound less precise at first. In reality, it is usually the most accurate way to diagnose perimenopause.
Doctors generally diagnose perimenopause clinically, which means they use the full pattern of your health history rather than trying to force the answer out of a single lab value. Guidance from the American College of Obstetricians and Gynecologists reflects this approach. Age, menstrual changes, and symptoms usually carry more weight than one hormone result. Tests still have a place, especially if your symptoms begin before 40 or if another condition needs to be ruled out.
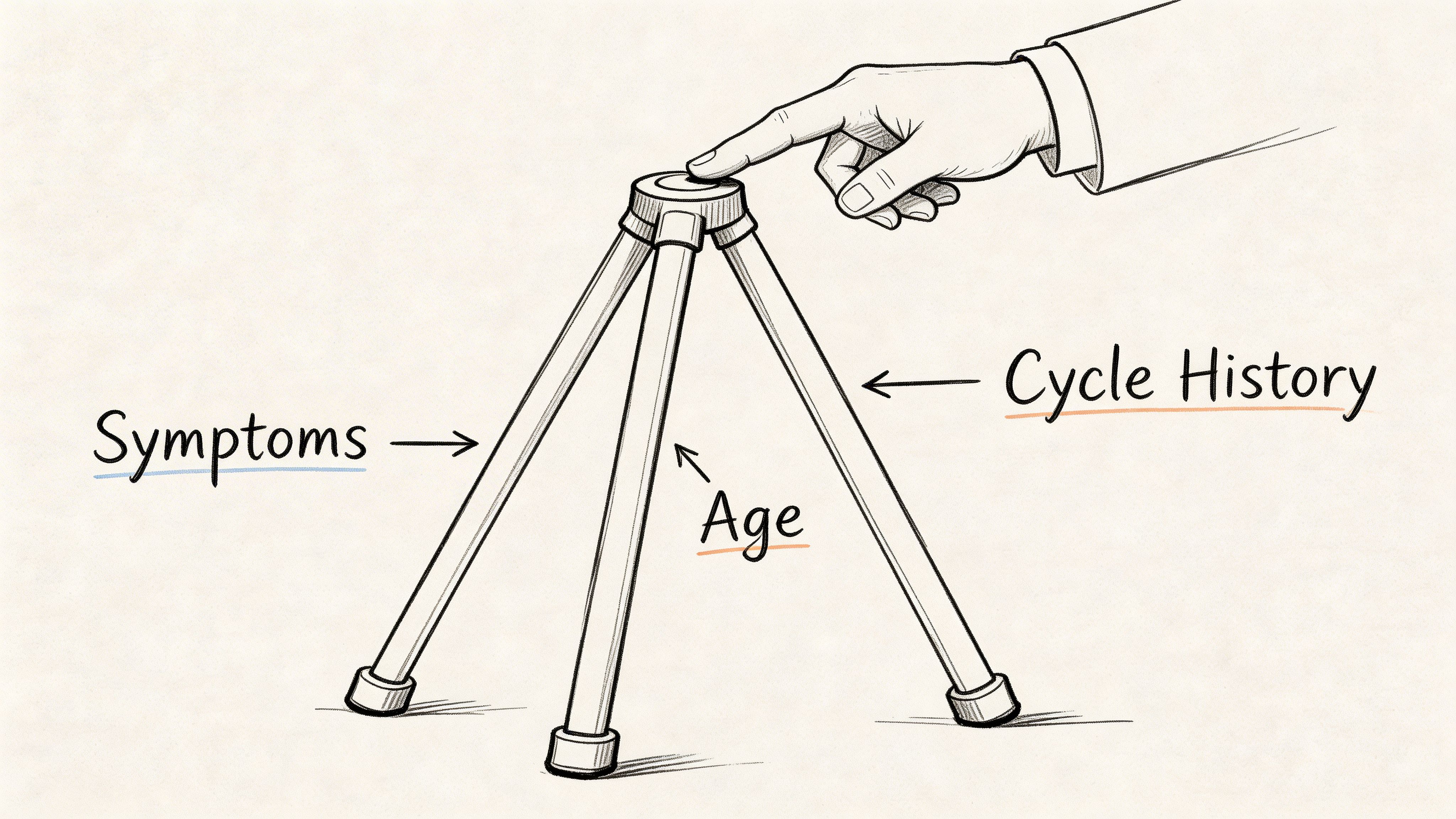
The three pillars doctors rely on
A perimenopause diagnosis is built from three kinds of information that make more sense together than they do alone.
Age. Symptoms in the 40s and early 50s usually fit a different clinical picture than the same symptoms in someone much younger.
Cycle history. Doctors look for shifts in timing, flow, skipped periods, spotting, or cycles that suddenly become less predictable.
Symptoms. Hot flashes, night sweats, sleep disruption, mood changes, vaginal dryness, brain fog, and lower energy can all add to the pattern.
This is one reason a single hormone test often falls short. A blood draw captures one moment. Perimenopause is a moving process.
Why your story carries real diagnostic weight
Your symptom history is not a backup plan in case testing fails. It is often the main evidence.
A helpful way to frame it is the ocean analogy from earlier. One lab result is like a single photo of rough water. It may show a wave, but it cannot show whether the tide has been changing for months. Your cycle changes and symptom pattern provide that longer view, which is why doctors ask so many detailed questions.
That is also why bringing specifics matters. “I feel off” is real, but “my periods went from every 28 days to every 21, I wake at 3 a.m. sweating, and my patience is much lower the week before bleeding” gives your clinician something they can use.
There’s also a practical reason to keep up with regular well-woman exams. These visits create space to discuss bleeding changes, pelvic symptoms, sleep problems, and preventive care in one conversation.
A short explainer may help this click:
▶ PlayWhat this means for you
If you have been waiting for a doctor to confirm perimenopause with one definitive test, it helps to reset the expectation.
The goal is an accurate pattern match that leads to good care. In many cases, a clear timeline of symptoms, cycle changes, and daily impact is more medically useful than a normal-looking hormone panel. That is also why symptom tracking can become so powerful, especially when an app like Lila helps you spot patterns you might miss in real time.
The Power of Tracking Your Symptoms and Cycle
If a hormone test is one photo of the ocean, tracking is the full film.
That’s what makes it so useful. Instead of asking your body to summarize months of change in one blood draw, you gather the pattern over time.
This matters on a large scale, too. 75 million U.S. women are currently in a menopausal state, and 1.3 million enter it annually, which helps explain why tools that centralize tracking are becoming more important for day-to-day management, according to this PMC article on menopause care and digital support.
What to track
You do not need a perfect spreadsheet. You need consistency.
A simple notebook works. A notes app works. A dedicated symptom tracker works even better if it helps you stay regular. Focus on patterns such as:
Cycle timing. When bleeding starts, how long it lasts, whether it’s lighter, heavier, or skipped.
Sleep. Trouble falling asleep, waking at night, early waking, and whether night sweats are involved.
Mood and stress tolerance. Irritability, anxiety, low mood, tearfulness, feeling unusually overwhelmed.
Body symptoms. Hot flashes, breast tenderness, headaches, joint aches, bloating, vaginal dryness.
Energy and cognition. Afternoon crashes, brain fog, word-finding trouble, feeling “off.”
Possible triggers. Alcohol, poor sleep, stress, spicy food, illness, travel.
Why tracking beats guessing
Tracking turns vague memory into usable information.
Without tracking, many women arrive at an appointment saying, “I think my periods are getting weird” or “I haven’t been sleeping well lately.” Those are honest statements, but they’re hard to analyze. With tracking, the conversation becomes more precise. Your cycle shortened, then stretched out. Sleep worsened before bleeding changes. Hot flashes clustered on certain days. Mood symptoms became less random than they felt.
The pattern is often more revealing than any individual symptom.
Tracking also helps you notice what improves things. If reducing alcohol, adjusting exercise timing, or improving stress management helps, that’s valuable. If stress seems to be making everything louder, resources on how to reduce cortisol levels naturally can support the broader picture without pretending stress is the only issue.
What makes digital tracking different
Paper journals are useful, but they can become hard to review.
That’s where apps can help. A strong tracker brings symptoms, cycle data, sleep, and mood into one place so you can spot trends faster and bring cleaner information to your clinician. If you want a sense of what that looks like, this overview of a menopause symptom tracker app shows how digital logging can organize details that are difficult to hold in your head.
The key idea is simple. You are not waiting for a test to tell you what’s happening. You are building a record that makes what’s happening easier to see.
How to Prepare for Your Doctor Visit
A good appointment starts before you walk in.
If symptoms are disrupting your life, if bleeding has changed a lot, or if you’re under 40 and having menopause-like symptoms, it’s worth booking a visit. The goal is not to ask for “the test.” The goal is to bring a clear picture and ask focused questions.
What to bring
Bring a short record covering the last few months, even if it’s imperfect.
Include:
Your cycle notes. Dates, skipped periods, heavier or lighter bleeding, unusual spotting.
Your most disruptive symptoms. Pick the top three. Sleep, hot flashes, anxiety, brain fog, vaginal dryness, whatever is affecting you most.
Timing patterns. Did symptoms start before periods changed, or after?
A medication and supplement list. Include anything new.
Questions worth asking
You don’t need a long script. A few direct questions are enough.
Could this pattern fit perimenopause?
Do my symptoms suggest that we should rule out anything else, such as thyroid problems?
If testing won’t confirm perimenopause, what would testing help us evaluate?
What treatment options match my most bothersome symptoms right now?
What changes would make you want me to follow up sooner?
How to make the visit more productive
If you tend to freeze up in appointments, write your main concerns down in advance.
A helpful structure is one sentence for what changed, one sentence for how it affects daily life, and one sentence for what you want help with. For example: “My periods have become irregular, I’m waking several times a night, and I want help figuring out whether this is perimenopause and what to do next.”
That gives your clinician something practical to work with.
Frequently Asked Questions About Perimenopause Tests
Are at-home perimenopause tests useful
They can add a little context, but they rarely give a clear answer on their own.
The main problem is timing. Perimenopause hormones can shift from day to day, so one home test can work like a single photo of a rough ocean. It captures one moment, not the overall pattern. Even kits that use more than one sample are still giving you a partial snapshot.
That means an at-home test may be mildly informative, especially if you are curious about FSH trends. It should not be treated as a diagnosis.
What if I’ve had a hysterectomy and can’t track periods
This situation is trickier because one of the biggest clues, cycle change, is missing.
In that case, an at-home multi-day hormone kit may be a little more useful than it is for someone who can still track periods. It can add one piece of objective information. But your symptom pattern still matters more than any single result. Doctors often rely on age, symptom history, sleep changes, hot flashes, mood shifts, vaginal symptoms, and other factors to judge whether perimenopause is the likely explanation.
If tests don’t diagnose perimenopause, why would a doctor order them
Because your clinician may be checking for other causes of the same symptoms.
Hot flashes, fatigue, sleep disruption, anxiety, brain fog, and cycle changes can overlap with thyroid disorders, pregnancy, medication effects, or other health issues. The North American Menopause Society explains that hormone testing is often unnecessary for diagnosing perimenopause, but other lab work may be helpful when the picture is unclear or symptoms suggest another condition: Menopause.org overview of perimenopause.
So the purpose of testing is often clarification, not confirmation.
Can I still be in perimenopause if my test was normal
Yes.
A normal hormone result does not rule it out. This confuses many women because we are used to tests giving yes-or-no answers. Perimenopause usually does not work that way. If your symptoms and timing fit, a “normal” result may mean the test caught your hormones on a quieter day.
What is the most reliable next step
Start tracking patterns.
Write down cycle changes if you still have periods, along with hot flashes, sleep problems, mood changes, headaches, vaginal dryness, libido shifts, and anything else affecting daily life. Over a few months, that record often becomes more useful than a one-time lab value because it shows the trend, not just a moment.
If you want a simpler way to track symptoms, cycles, sleep, mood, and daily patterns in one place, Lila can help you turn confusing changes into something clear and actionable. Instead of chasing a single test result, you can build a useful record of what your body is doing and use that information to make better decisions about support, treatment, and next steps.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.