Estriol vs Estradiol: Which Is Right for Menopause?
Confused about estriol vs estradiol for menopause relief? Our guide compares potency, safety, and uses to help you and your doctor decide on the best HRT.

You open your symptom tracker to check whether last night was another fluke. Sleep was broken again. Your afternoon bloating showed up for the fourth day this week. Two hot flashes hit during a meeting. Mood dipped hard before dinner. Sex has started to feel uncomfortable, but not every time. The pattern is there, yet it still doesn’t point to one simple answer.
That’s often the moment the estriol vs estradiol question shows up.
Online, the conversation gets messy fast. One side presents estradiol as the standard. Another treats estriol like the gentler, smarter option for everyone. Neither framing is very helpful when you’re the person trying to decide what to do with real symptoms, real trade-offs, and a real medical history.
If you're still sorting out the broader role of hormone therapy, this overview of hormone therapy for menopause is a useful starting point before narrowing in on which estrogen makes sense.
The practical answer is this. Estradiol and estriol are not interchangeable, and the better choice depends less on ideology than on symptom pattern. If your problem is whole-body menopause symptoms, one option usually makes more clinical sense. If your symptoms are mainly vaginal or urinary, the other may be more appropriate. If weight gain and bloating are part of the picture, the conversation gets more nuanced, because the evidence there is thinner than most marketing suggests.
Navigating the Crossroads of Menopause Hormone Therapy
A common scenario in clinic looks like this. A woman in her late 40s brings a careful record of several months of symptoms. Her cycles have become less predictable. She’s waking at 3 a.m., then dragging through the next day. She feels puffy, more reactive, and less resilient. She may also have vaginal dryness or urinary irritation, but those symptoms don’t always come up first because hot flashes, anxiety, and sleep disruption are louder.
Then she starts reading.
She learns that estradiol is widely prescribed. She also sees claims that estriol is weaker and therefore safer. She hears the word “bioidentical” used in different ways. She reads strong opinions about compounded hormones, patches, creams, and vaginal products. By the time she books an appointment, the question isn’t just “Should I use estrogen?” It’s “Which estrogen, in what form, and for which symptoms?”
Clinical reality: The best hormone plan usually starts with identifying the dominant symptom cluster, not with picking the most popular hormone online.
That distinction matters. Menopause symptoms don’t arrive in neat categories, but they do tend to cluster. Some women have classic systemic symptoms such as hot flashes, night sweats, mood instability, and sleep disruption. Others mainly struggle with genitourinary symptoms such as dryness, irritation, painful intercourse, or recurrent urinary discomfort. Some have both.
Estriol vs estradiol is really a question about targeting. Are you trying to influence the whole body, or a specific local tissue? Are you treating moderate to severe symptoms, or milder, focused ones? Are you prioritizing potency, regulation, and standardization, or are you trying to minimize systemic exposure where possible?
Those are the right questions. They lead to far better decisions than the simplistic idea that one hormone is always “better.”
Understanding the Two Key Estrogens in Your Body
Before comparing therapies, it helps to know what these hormones are doing naturally.
Estradiol (E2) and estriol (E3) are both forms of estrogen. The body makes other estrogens too, but these two drive most of the estriol vs estradiol discussion in menopause care.
Estradiol is the workhorse
Estradiol is the body’s main active estrogen during the reproductive years. It’s the hormone most clinicians think about when they’re addressing broad menopausal symptoms because it has strong effects across multiple tissues.
Verified data describes estradiol as the most potent natural estrogen, approximately 10 to 12 times stronger than estriol, and the primary estrogen produced by the ovaries during reproductive years. The same source notes that estradiol is commonly used in FDA-approved hormone replacement therapy for postmenopausal women managing systemic symptoms such as hot flashes and other menopause-related complaints (SingleCare on estriol vs estradiol).
That’s why I often describe estradiol as the workhorse estrogen. It has enough potency to affect the brain, bones, vasomotor system, and vaginal tissue. When someone has multiple menopause symptoms happening at once, estradiol is usually the hormone doing the heavy lifting in treatment.
For women who are trying to understand where they stand hormonally before or during treatment discussions, an Estradiol Test can be a useful conversation tool with a clinician, especially when symptoms and cycle changes are hard to interpret.
Estriol is the specialist
Estriol plays a very different natural role. It is the weakest of the three main estrogens and becomes most prominent during pregnancy. Outside pregnancy, its levels are much lower.
That physiological role tells you something important. Estriol isn’t built for broad, sustained, whole-body estrogen effects in the way estradiol is. It behaves more like a gentle specialist than a workhorse.
A simple way to think about it is this:
Hormone | Core role in the body | Clinical personality |
|---|---|---|
Estradiol (E2) | Main active estrogen in reproductive years | Strong, systemic, versatile |
Estriol (E3) | Dominant in pregnancy, low otherwise | Weaker, gentler, more localized |
Why this matters in menopause
This difference isn’t academic. It shapes what each hormone can realistically do in treatment.
When women compare estriol vs estradiol, they’re often really asking one of these questions:
“Which one is stronger?” Estradiol.
“Which one acts more gently?” Estriol.
“Which one is used more often in standard menopause care?” Estradiol.
“Which one fits better for local vaginal symptoms?” Often estriol, depending on the clinical context.
Estradiol is the hormone you consider when menopause feels like it has taken over the whole body. Estriol is the hormone you consider when the problem is narrower and more local.
That mental model helps. It keeps the conversation grounded before you get pulled into debates about branding, compounding, and internet claims that overpromise.
How Potency and Receptor Activity Create Different Effects
The reason estriol vs estradiol feels like such a big choice is that these hormones don’t just differ in strength. They interact with the body differently.
The receptor piece that changes everything
Estrogen works by binding to estrogen receptors. The two main ones are ERα and ERβ. Different tissues contain different mixes of these receptors, which is one reason an estrogen can feel broad and powerful in one setting and milder in another.
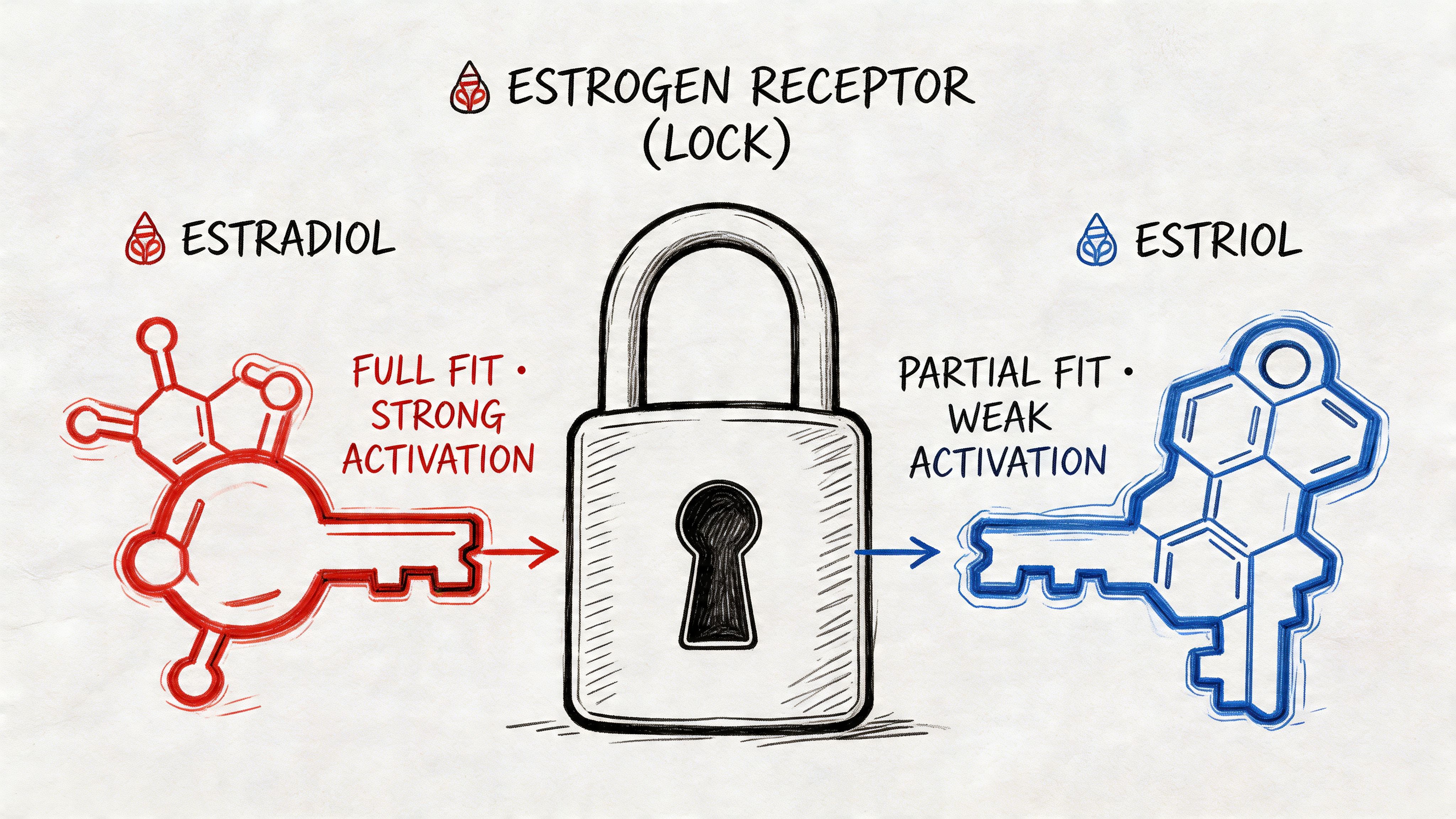
Verified data shows that estradiol binds strongly to both ERα and ERβ with relative binding affinity set at 100%, while estriol binds much more weakly, at 11.3% to ERα and 17.6% to ERβ. That same source explains that this receptor profile drives different outcomes. Estradiol functions as a systemic hormone, while estriol is used primarily for localized application (Health Natura on receptor activity).
What that means in plain language
If estradiol is a master key, estriol is more like a limited-access key.
Estradiol binds strongly enough to influence many tissues at once. That’s why it’s used for symptom clusters that include hot flashes, night sweats, mood changes, and bone-related concerns. It’s not subtle. That’s often exactly why it works.
Estriol has weaker receptor binding and tends to fit better when the treatment goal is local tissue support rather than broad hormonal replacement. In practice, that usually means vaginal and urinary symptoms.
Here’s the practical distinction:
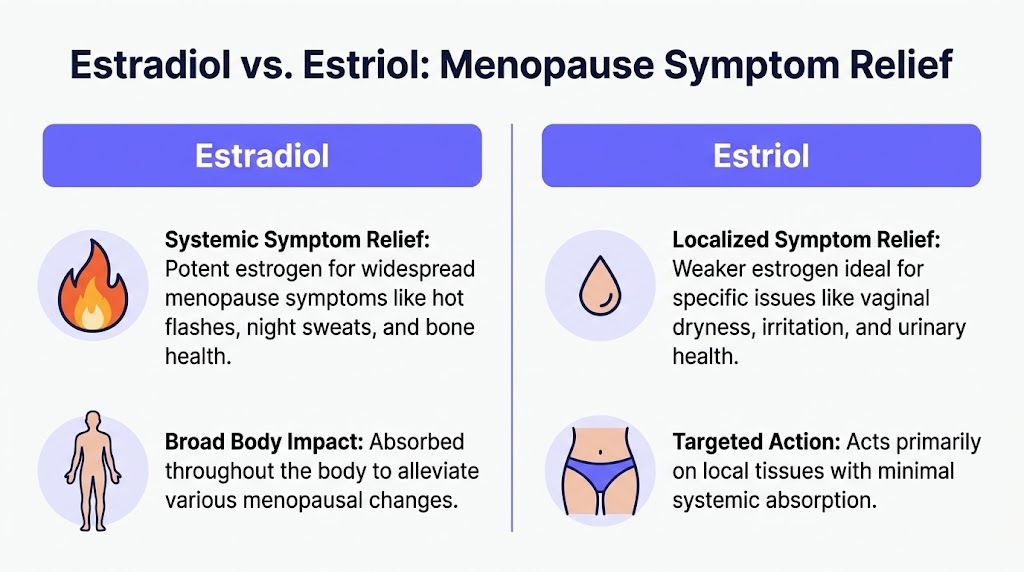
Estradiol is usually the better match when symptoms are widespread.
Estriol is usually considered when symptoms are concentrated in vaginal or urinary tissues.
Using a weaker hormone doesn’t automatically mean better treatment. It means less hormonal force, which can be an advantage or a limitation depending on the goal.
Why some symptoms improve and others don’t
Many women find themselves frustrated when they start a local estrogen product hoping it will help sleep, anxiety, or hot flashes, then feel disappointed when it doesn’t do much. That’s not necessarily treatment failure. It may be a mismatch between the product and the symptom cluster.
A local therapy can help local tissue. It usually won’t do the same job as a systemic one.
If your symptoms involve the brain, sleep, temperature regulation, and mood all at once, a local vaginal hormone won’t usually solve the whole problem.
On the other hand, many women don’t need broad systemic treatment if their main complaint is vaginal dryness, irritation, or discomfort with sex. In that setting, using a gentler, more localized option can be a very rational strategy.
Potency is not the same as quality
Patients sometimes hear that estriol is “natural” and estradiol is “strong,” then assume strong means harsh or unsafe. That’s too simplistic.
Potency tells you how much biological effect a hormone is likely to have. It doesn’t tell you whether the treatment is right or wrong. A more potent hormone can be the best choice when the symptom burden is high. A weaker hormone can be the better choice when the target is narrow and safety priorities favor less systemic exposure.
The useful question isn’t “Which hormone is best?” It’s “Which receptor pattern and delivery style matches what my body is doing?”
Comparing Estradiol and Estriol for Menopause Symptoms
If you want the shortest practical answer to estriol vs estradiol, it’s this: estradiol is usually chosen for systemic menopause symptoms, and estriol is usually considered for localized vaginal and urinary symptoms.
That sounds simple, but the details matter.
Here’s the side-by-side view early, because most women are trying to make sense of this clinically, not philosophically.
Key differences at a glance
Feature | Estradiol (E2) | Estriol (E3) |
|---|---|---|
Relative potency | Most potent natural estrogen | Weaker estrogen |
Primary use pattern | Systemic symptom relief | Localized symptom relief |
Common symptom targets | Hot flashes, night sweats, mood changes, bone-related concerns, vaginal symptoms in some forms | Vaginal dryness, irritation, painful intercourse, urinary symptoms |
Regulatory status in the U.S. | Available in FDA-approved formulations | Not FDA-approved for human use, commonly accessed through compounding |
Typical formulations | Tablets, patches, creams, vaginal tablets, rings | Compounded creams, suppositories, other local vaginal preparations |
Best-fit patient pattern | Multi-system menopause symptoms | Isolated or predominantly genitourinary symptoms |
When estradiol is usually the better fit
Estradiol is the standard option when symptoms are broad and disruptive. That includes women who report hot flashes, sleep disruption, mood swings, and a sense that their whole system is off.
Its strength is also its purpose. Estradiol is used because it can reach beyond the vagina and affect the wider symptom network that declining estrogen can create.
In practice, estradiol often makes the most sense when you’re seeing symptom patterns like:
Daily vasomotor symptoms such as hot flashes or night sweats
Sleep problems that track with temperature changes or hormonal instability
Mood volatility that seems hormonally linked
Bone-health concerns where systemic estrogen is part of the discussion
Mixed symptom patterns that include both vaginal and whole-body complaints
If mood symptoms are prominent, it can help to understand how hormonal shifts intersect with mental health. This overview of why perimenopause can cause depression gives useful clinical context for that part of the picture.
When estriol may make more sense
Estriol fits a narrower lane. Verified data describes estriol as the weakest of the three main estrogens, rising dramatically during pregnancy but remaining low otherwise, and notes that its short half-life and weak receptor binding make it unsuitable for systemic HRT but ideal for localized vaginal therapy. The same source reports 60% to 80% symptom relief for mild to moderate dryness and urinary issues in studies of local use (Evvy on estriol vs estradiol).
That makes estriol a reasonable option when the main problems are:
Vaginal dryness
Irritation or burning
Pain during intercourse
Urinary discomfort or recurrent irritation
A desire to target tissue locally rather than treat the whole body
Here’s a short explainer if you want a visual summary before going deeper:
▶ PlayWhat doesn’t work well
Some expectations need correcting.
Estriol is not a reliable stand-in for systemic menopause therapy when someone has significant hot flashes, strong sleep disruption, and mood instability. It may help a local symptom while leaving the major drivers untouched.
Estradiol is not always necessary when the only problem is vaginal dryness or discomfort with sex. Using a systemic hormone for a local problem can be more treatment than some women need.
The right treatment often feels less like choosing a better hormone and more like choosing the right delivery range.
The confusion in estriol vs estradiol discussions usually comes from treating all menopause symptoms as if they come from one bucket. They don’t. Menopause care works better when symptoms are grouped by pattern, then matched to a therapy that targets that pattern.
Safety Profiles Formulations and Medical Monitoring
Safety discussions around estriol vs estradiol often get distorted by fear on one side and oversimplified reassurance on the other. The practical view is more balanced. Both can be useful. Neither should be chosen casually.
What safety looks like in real use
Estradiol’s greater potency is one reason it helps more with broad symptoms. It’s also why clinicians pay closer attention to route, dose, and whether progesterone is needed in women who still have a uterus.
Estriol’s weaker action may reduce some concerns related to stronger tissue stimulation, which is part of its appeal. But “weaker” doesn’t mean “monitoring not required,” especially when treatment is compounded and standardization can vary.
A useful point from the comparative data is that local therapies still deserve proper follow-up. In a 24-week randomized controlled trial comparing estradiol vaginal tablets with estriol vagitories for atrophic vaginitis, both improved symptoms. The estradiol group had better tolerability on several measures, with 6% reporting urinary leakage versus 65% in the estriol group, and both groups showed increases in endometrial thickness during daily use, 1.1 mm with estradiol and 0.5 mm with estriol, which resolved when dosing was reduced to twice weekly (PubMed trial summary).
That trial is helpful because it corrects a common misunderstanding. Even “local” therapy isn’t outside the rules of clinical monitoring.
Common formulations and what they’re good at
Form matters almost as much as hormone choice.
Estradiol formulations
Estradiol is available in several FDA-approved forms, including tablets, patches, creams, and vaginal products such as Estrace, Vivelle-Dot, Vagifem, and Climara, according to the verified data cited earlier.
That gives clinicians flexibility. A patch may be chosen for steady systemic delivery. A vaginal tablet or cream may be chosen when vaginal symptoms are part of the picture. If you’re considering transdermal therapy specifically, this guide to the benefits of estradiol patch is a practical read.
Estriol formulations
Estriol is typically encountered through compounding pharmacies rather than FDA-approved human products in the U.S. In practice, that usually means local vaginal formulations such as creams or suppositories.
The trade-off becomes evident. Compounding can allow customization, but it also means you’re not using the same level of FDA-approved standardization available with many estradiol products.
What monitoring should include
Good follow-up isn’t just about lab work. It’s also about tracking the symptoms the hormone is supposed to improve, and watching for symptoms it might worsen.
A reasonable clinical conversation usually includes:
Symptom response such as changes in hot flashes, sleep, dryness, discomfort, or urinary irritation
Bleeding patterns especially if any unexpected vaginal bleeding appears
Breast symptoms including tenderness or changes that need evaluation
Tolerability such as bloating, headaches, breast fullness, or irritation at the application site
Uterine protection if estradiol is used systemically in someone with a uterus
Bring specific observations, not a vague impression that you “feel off.” The more precise the symptom pattern, the easier it is to adjust therapy well.
What patients often underestimate
Many women focus on the hormone name and ignore the delivery method. That’s a mistake.
A hormone’s effect changes with where it goes, how much is absorbed, and what symptom it’s meant to treat. A patch, vaginal tablet, compounded cream, and oral tablet are not interchangeable just because they all involve estrogen.
That’s also why copying another woman’s regimen rarely works well. The right choice depends on symptom distribution, health history, and how closely the treatment’s reach matches the problem.
How to Match the Right Hormone to Your Symptoms
Symptom tracking becomes useful when it changes the treatment question from “Which hormone is better?” to “Which hormone matches the pattern I’m seeing?”
Match the therapy to the cluster
If your records show hot flashes, night waking, mood swings, and a sense of whole-body hormonal instability, systemic estradiol is usually the more evidence-based place to start. Those symptoms suggest a broad estrogen deficit pattern, not a local tissue issue.
If your records show vaginal dryness, irritation, discomfort with sex, or urinary irritation, and you don’t have prominent systemic symptoms, local therapy often makes more sense. That’s where estriol can enter the conversation as a focused option.
If you have both sets of symptoms, some clinicians use a combined strategy. The local symptom may need local treatment even when systemic therapy is also on board.
A practical symptom map
Use your tracked symptoms this way:
Frequent hot flashes plus broken sleep point more toward systemic treatment considerations.
Dryness plus painful intercourse without major vasomotor symptoms points more toward localized vaginal therapy.
Mood symptoms plus temperature dysregulation usually deserve a broader hormonal conversation.
Urinary irritation that keeps recurring may reflect genitourinary tissue changes rather than infection alone, which changes the treatment approach.
Mixed symptoms with bloating and weight changes require more nuance, because the estrogen choice may not fully explain what’s happening metabolically.
The metabolic question women keep asking
This is the most under-discussed part of estriol vs estradiol.
Women often want to know whether one hormone is less likely to worsen weight gain, puffiness, or insulin-related changes. The marketing around this gets ahead of the evidence.
Verified data notes that estradiol may promote fat storage through ER-alpha effects, while estriol’s beta-receptor preference could theoretically support lean mass without visceral fat accrual. But the same source is clear that no studies test this in women in their 40s to 50s, and that human trials are lacking. It also notes that 2026 preclinical data showed estriol improving glucose uptake 15% better in adipose models versus estradiol, but this is preclinical rather than human outcome data (Cleopatra Rx on metabolic questions).
That means two things can be true at once:
There’s a plausible biologic reason people are asking whether estriol might be more “metabolic-friendly.”
We do not have strong human evidence to promise that it will lead to less weight gain or less bloating.
Don’t let anyone sell certainty where only theory exists.
What to do with bloating and weight changes
If these are major concerns, track them with the same seriousness you’d track hot flashes.
Helpful categories include:
Daily abdominal bloating
Morning scale trends
Waistband fit
Appetite shifts
Energy after meals
Sleep quality
Constipation or bowel changes
Why? Because weight and bloating in midlife are rarely explained by estrogen choice alone. Sleep disruption, stress physiology, changes in activity, cycle variability, and food tolerance all affect the picture. A hormone may help indirectly by improving sleep or stabilizing symptoms. It may also produce side effects that feel like fluid retention or breast fullness. The point is to observe the response rather than assume the theory will predict your outcome.
The smartest way to use hormone decisions
Use estriol vs estradiol as a targeting framework, not a loyalty test.
Ask:
Is the problem local or systemic?
Are the symptoms mild and focused, or broad and disruptive?
Is safety concern driving the plan?
Is the main frustration hot flashes and sleep, or dryness and urinary discomfort?
Are metabolic complaints part of the story, and am I tracking them carefully enough to tell what changes after treatment?
That line of thinking usually leads to better care than chasing whichever hormone currently sounds cleaner online.
Preparing for a Productive Conversation With Your Clinician
The best menopause visits are collaborative. They work better when you walk in with patterns, not just frustration.
What to bring to the appointment
Bring a concise symptom record that shows timing, severity, and clusters. Your clinician does not need pages of raw notes. They need a usable summary.
Include things like:
Most disruptive symptoms such as hot flashes, insomnia, vaginal dryness, low mood, bloating, or urinary irritation
When they occur including whether they cluster around sleep, cycle changes, or certain times of day
What has already been tried such as lubricants, vaginal moisturizers, supplements, or prior hormone use
Any bleeding changes especially if they are new or unpredictable
Your treatment goals such as sleep improvement, pain-free sex, fewer hot flashes, or less day-to-day puffiness
If you’re still sorting out whether your symptoms fit perimenopause or menopause, this guide on how to test for menopause can help you prepare for that discussion.
Questions worth asking directly
Good questions make the visit more specific. Try these:
Based on my symptom pattern, does systemic estradiol or localized estrogen therapy make more sense?
If my symptoms are mainly vaginal or urinary, would estriol be a reasonable option for me?
If I still have a uterus, do I need progesterone with the plan you’re recommending?
What are the pros and cons of FDA-approved estradiol versus compounded estriol in my case?
What side effects should make me contact you sooner?
How will we judge whether this is working?
If bloating or weight changes are a major concern for me, how should I track them after starting treatment?
What a strong treatment plan sounds like
A solid plan is specific. It explains why this hormone, why this route, and what success should look like over the next phase of care.
You should leave knowing:
What symptom the treatment is meant to improve first
How to use it correctly
What changes are expected
What changes are not expected
When follow-up should happen
What symptoms require reassessment
A good hormone conversation leaves you with a monitoring plan, not just a prescription.
The main mindset shift
You don’t need to walk into the visit already knowing whether estriol or estradiol is right. You do need enough clarity to describe your symptom pattern accurately and ask targeted questions.
That’s especially important because the estriol vs estradiol decision is rarely about one symptom in isolation. It’s about matching the treatment’s reach to the life disruption you are experiencing. Women who come prepared with symptom trends, questions, and goals usually get better, more individualized care than women who ask for “something for menopause.”
If you want a clearer picture of your symptom patterns before your next appointment, Lila can help you track hot flashes, sleep, mood, bloating, weight changes, meals, and cycles in one place. That kind of organized, day-to-day data can make hormone decisions far more precise, especially when you're trying to sort out whether your symptoms point toward localized relief, systemic treatment, or a more nuanced plan.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.