7 Exercises to Avoid During Menopause
Discover the 7 exercises to avoid during menopause. Learn why they can worsen symptoms and find safer, effective alternatives for your fitness routine.

“Work out harder” is often the worst advice a menopausal body can get.
What changes in midlife is not motivation. It is physiology. Lower estrogen can affect bone density, tendon stiffness, joint comfort, pelvic floor support, sleep quality, and heat regulation. A workout that used to feel productive can suddenly leave you with pounding joints, urinary leaking, poor recovery, a nighttime hot flash, or that wired-tired feeling that makes the next day harder.
I see this often in practice. Women assume the problem is inconsistency or lack of effort, when the actual issue is a mismatch between the training stress and the body’s current tolerance. More intensity is not always more benefit, especially if symptoms spike later.
That is why this article focuses on specific exercise categories that can backfire during menopause, and the reasons they do. The goal is not to make movement smaller. The goal is to make it more targeted, so you can keep building strength, cardiovascular fitness, and confidence without paying for it with worse symptoms.
Heat is one of the clearest examples. Hard sessions that raise core temperature quickly can be uncomfortable for women who are already dealing with thermoregulatory shifts in perimenopause and menopause. For some, the workout itself is manageable, but the aftermath is not. Sleep worsens, flushing shows up later, or recovery drags.
The better question is: which exercises give you enough training stimulus without pushing your joints, pelvic floor, or nervous system past what they can recover from right now?
That answer is personal, and patterns matter. Tracking what happened during the workout and how you felt afterward often reveals more than willpower ever will. If you need a starting point for what tends to work better, this guide to the best exercises for menopause is a useful companion to the exercises covered here.
If running is part of your routine, it also helps to review practical running injury prevention strategies before you decide what stays and what goes.
1. High-Impact Plyometric Exercises
Jump squats, box jumps, burpees, tuck jumps, and many boot camp drills ask your joints, pelvic floor, and nervous system to absorb force quickly. During menopause, that’s often too much load for too little payoff. If you already notice knee soreness, hip irritation, or leaking with impact, plyometrics usually magnify the problem instead of fixing it.
The issue isn’t that explosive training is always “bad.” The issue is that declining estrogen can leave bones and connective tissues less tolerant of repeated hard landings. For women with osteoarthritis or osteoporosis, jumping and plyometrics can inflame joints through compression forces, and postmenopausal guidance specifically warns against high-impact aerobics and fall-prone activities.
What usually goes wrong
In real life, this shows up in classes that cycle through jump lunges, burpees, and box work while music is loud and transitions are rushed. Form slips fast when fatigue hits. Landing mechanics get sloppy, breathing gets shallow, and the workout turns into impact practice rather than strength training.
If you’re doing CrossFit-style metcons or HIIT circuits with repeated jumping, you may also notice a second problem: symptom spillover later in the day. Some women feel fine during class, then get joint stiffness, poor sleep, or an increase in heat symptoms afterward.
Practical rule: If an exercise leaves you feeling pounded rather than trained, it’s probably too impact-heavy for your current stage.
A better swap is controlled resistance work paired with low-impact conditioning. Think goblet squats instead of jump squats, step-ups instead of box jumps, and brisk incline walking, cycling, swimming, or water aerobics instead of burpee intervals. If you want ideas for that shift, Lila’s guide to the best exercises for menopause is a useful starting point.
Choose force you can control: Slow squats, split squats, and Romanian deadlifts build strength without repeated hard landings.
Use intensity without impact: Stationary bike pushes, rowing, or pool intervals can feel athletic without battering knees and hips.
Track the aftermath: In Lila, log the session type and note hot flashes, sleep, or next-day joint pain. Patterns usually show up quickly.
2. Heavy Overhead Weightlifting Without Proper Support
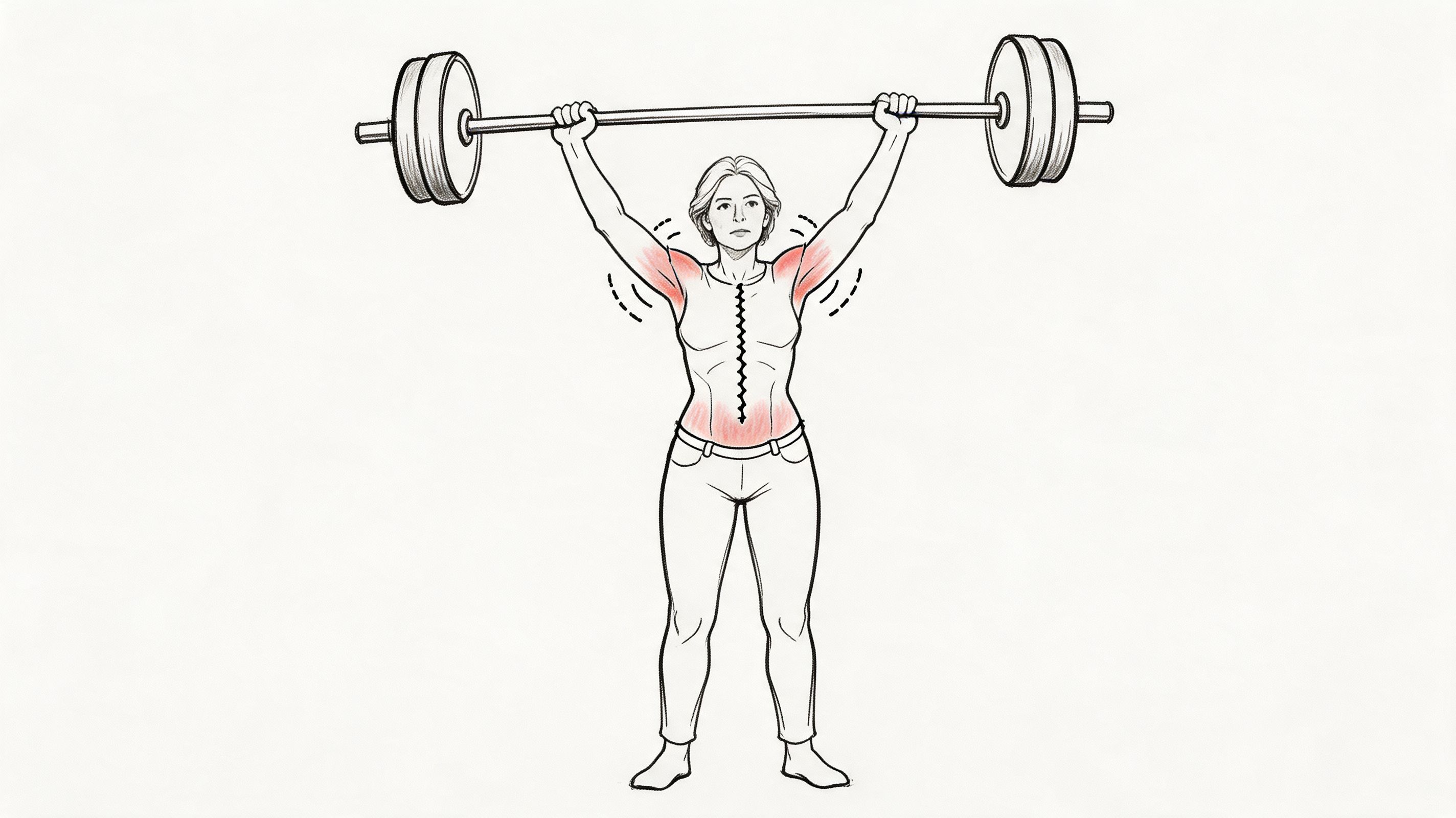
Overhead lifting is not automatically a bad idea during menopause. For many women, though, it is one of the first places where hormonal shifts expose weak links in mobility, pressure control, and recovery.
A heavy press, push press, snatch, or overhead squat asks for a lot at once. You need shoulder motion, thoracic extension, rib control, grip strength, and the ability to create enough trunk stiffness without turning every rep into a breath-holding contest. During menopause, that combination can become less forgiving. Joint irritation tends to show up faster, heat builds quickly, and pelvic floor symptoms are more likely to appear if you brace hard or bear down to finish the lift.
Resistance training still belongs in a menopause fitness plan. Research on exercise in postmenopausal women has found benefits for strength, bone health, and metabolic health in this review of exercise and bone-related outcomes in postmenopausal women. The trade-off is exercise selection and setup. Unsupported overhead loading is often the problem, especially if symptoms are already pointing to low back strain, neck tension, shoulder pinching, or heaviness through the pelvic floor.
I see this often with women who were strong lifters before menopause and try to return to old numbers on standing barbell presses. The determination is still there. The recovery margin is smaller.
Why overhead work can start bothering you now
Estrogen changes affect connective tissue, joint comfort, and tissue tolerance. That does not mean joints suddenly become fragile. It does mean a movement that used to feel stable can start feeling crowded or cranky if the shoulder blade does not rotate well, the upper back stays stiff, or the low back takes over.
The pressure piece matters too. Heavy overhead lifting often encourages breath-holding and aggressive bracing. For women dealing with leaking, prolapse symptoms, or abdominal pressure sensitivity, that strategy can make the session feel strong in the moment and leave them irritated later. If that pattern sounds familiar, it is worth reading more about menopause-related joint pain and movement tolerance.
Another issue is thermoregulation. Hard sets done overhead can spike effort quickly, especially in warm gyms or fast-paced classes. Women who are already dealing with hot flashes, poor sleep, or a wired feeling after training often tolerate chest-supported, seated, or half-kneeling variations much better than heavy standing barbell work.
If overhead work leaves you with neck tension, back arching, pelvic floor pressure, or a flushed, overcooked feeling, the setup is asking more from your system than it is giving back.
Better options still train the same general pattern. Seated dumbbell presses, landmine presses, half-kneeling single-arm presses, machine shoulder presses, and lat pulldowns let you build upper-body strength with more control and less compensation.
Use support intentionally: A bench, machine, or half-kneeling position reduces the chance that your low back and ribs will fake shoulder mobility.
Match the breathing strategy to the symptom picture: Exhale through the hardest part of the rep if breath-holding triggers leaking, pressure, or headaches.
Earn heavier overhead loading: If you cannot keep ribs stacked over pelvis and shoulders moving cleanly, lower the load and clean up the pattern first.
Track your response, not just the weight used: In Lila, log the variation, load, and any next-day signs like shoulder ache, hot flashes, or pelvic heaviness. That gives you a clearer way to spot whether overhead work is helping or just costing you recovery.
3. Intense Long-Distance Running
Distance running is not automatically a bad fit in menopause. The problem is that long, hard mileage is often treated as universally healthy, even when your recovery capacity, joint tolerance, and heat regulation have changed.
For many women, marathon-style training creates a triple hit. Repetitive impact can aggravate hips, knees, feet, or low back. Long efforts raise body temperature for too long in women who are already dealing with hot flashes or feeling overheated during exercise. High-volume endurance work also competes with strength training, sleep recovery, and day-to-day stress management.
That trade-off matters.
Why long runs can backfire during menopause
Estrogen changes affect more than periods. They also influence collagen, tendon stiffness, joint comfort, and how resilient tissues feel under repeated load. A run that felt fine five years ago may now leave you with achy ankles, irritated knees, or a flare in next-day stiffness, especially if you are also under-recovered.
Thermoregulation is another common limiter. Long runs, warm weather, and poor sleep are a rough combination. If you finish a run feeling drained, flushed for hours, or wired late into the evening, your training dose may be too high for your current symptom picture.
Then there is the recovery cost. Long-distance running is not just cardio. It takes time, glycogen, muscular endurance, and nervous system bandwidth. If your lifting numbers are falling, your sleep worsens after long runs, or your hot flashes spike on higher-mileage weeks, that pattern is worth respecting.
If sore hips, knees, or ankles are already part of the picture, Lila’s article on menopause joint pain can help connect those symptoms to your training choices.
Women who enjoy mind-body work alongside running often do better with a lower-impact recovery day. This guide to yoga for perimenopause is a practical place to start.
Smarter ways to keep running without paying for it later
A common pattern I see is this: weekday runs feel manageable, but the long weekend run triggers a bad night of sleep, increased hunger, heavy legs, and more joint soreness than usual. That is useful feedback. It usually means the weekly structure needs work, not that running has to disappear.
Shorter runs often work better than one heroic long session. Run-walk intervals, softer surfaces, and one or two cross-training days can preserve fitness with less symptom fallout. Strength training also deserves protection here because bone, muscle, and tendon health usually need more support during and after menopause, not less.
Cap the long run before symptoms escalate: Stop while recovery still feels manageable, not when pride says you should add another few miles.
Use cross-training strategically: Cycling, rowing, swimming, and the elliptical keep aerobic fitness up without the same impact load.
Watch the full symptom pattern: Track joint pain, overheating, sleep, mood, cravings, and energy the day after longer runs in Lila.
Adjust goals to the season you are in: A strong 5K or steady 10K block may serve your body better than chasing half-marathon volume during a high-symptom stretch.
If calorie burn is part of how you compare workouts, PlateBird's guide on crunch calories is a useful reminder that more effort is not always the same as better programming. During menopause, the best training plan is the one that builds fitness without driving symptoms harder.
4. Intense Core Work with Heavy Intra-Abdominal Pressure
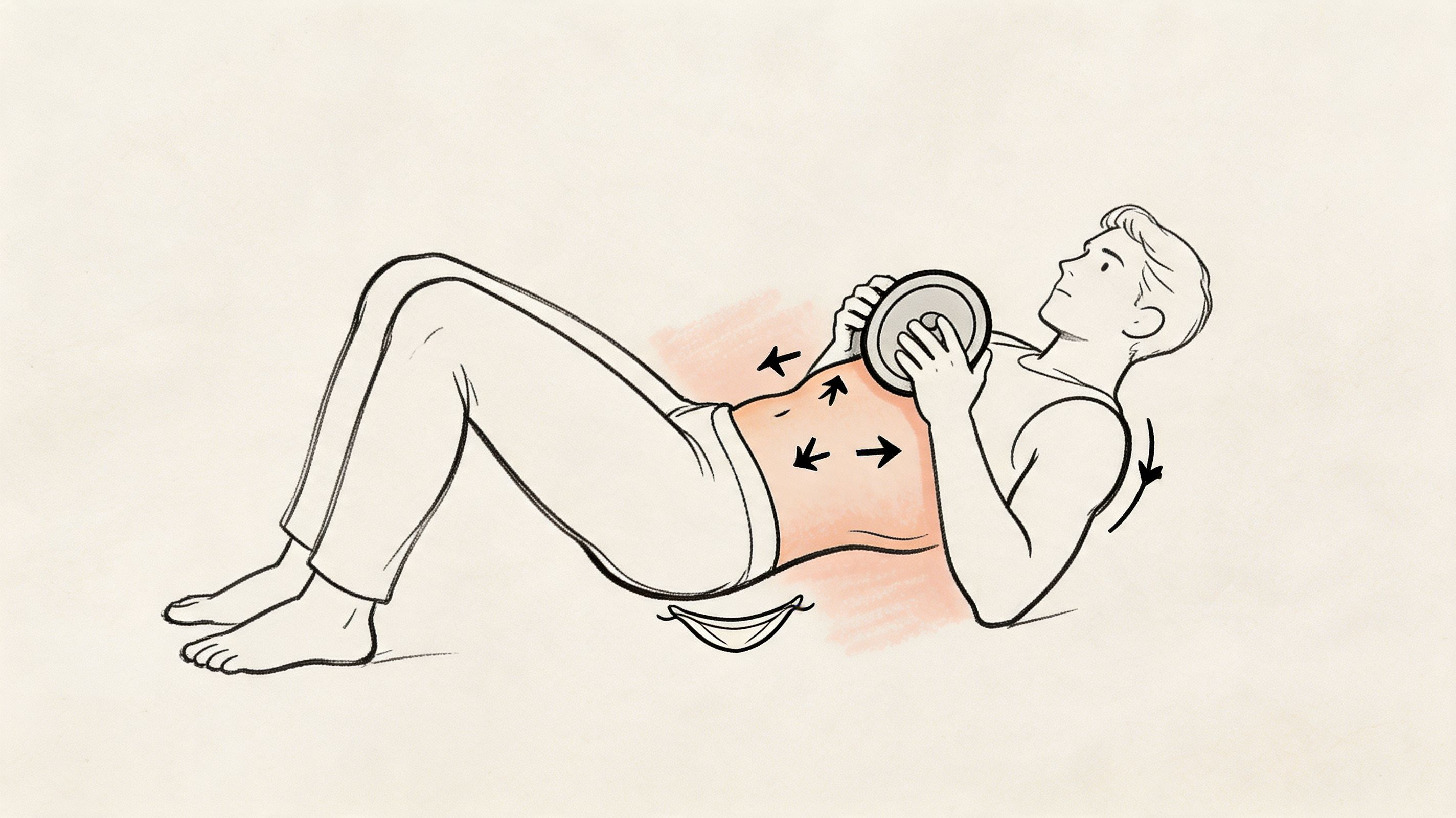
The old-school answer to “tone your middle” is still crunches, sit-ups, ab circuits, and long plank challenges. For many menopausal women, those are exactly the wrong tools. They often create too much pressure, too much spinal flexion, and too little carryover to real-life stability.
Postmenopausal guidance specifically warns against repeated trunk flexion exercises such as sit-ups or toe touches because they increase spinal loads and vertebral fracture risk. That warning becomes even more relevant if you have osteoporosis, osteopenia, back pain, or pelvic floor symptoms.
Why ab burnout isn’t the same as core strength
A heavy sit-up circuit can make your abs feel worked without teaching your trunk to manage pressure well. If you grip, bulge through the midline, hold your breath, or bear down to finish reps, the pelvic floor often takes the hit. That’s one reason some women notice leaking, pelvic heaviness, or low-back irritation after “core” classes.
Planks can create the same issue when they’re held to exhaustion. A technically solid short plank is a different exercise from a shaky, breath-held two-minute plank challenge.
Yoga and Pilates can help, but exercise selection matters there too. If you want a gentler entry point, Lila’s guide to yoga for perimenopause is more useful than copying social-media ab routines.
Strong core work should improve pressure control, not test how long you can strain.
The better alternative is deep-core and anti-movement work. Dead bugs, bird dogs, side planks with short holds, Pallof presses, and well-coached carries train the trunk to resist motion and coordinate with breathing. That tends to feel better in menopausal bodies and works better for daily life.
For anyone still using crunch volume as a measure of fitness, even consumer guides like PlateBird's guide on crunch calories show how often crunches get framed as a calorie-burn shortcut. That mindset misses the bigger issue. During menopause, pressure management matters more than ab burn.
Keep holds shorter: Short, clean sets beat long, shaky efforts.
Exhale on effort: Don’t hold your breath to finish reps.
Train stability patterns: Anti-rotation and anti-extension exercises usually have a better risk-reward ratio.
5. High-Intensity Interval Training at Maximum Effort Frequency
Many women are told to do more HIIT in menopause because it is time-efficient and good for metabolism. That advice misses a key detail. The dose that helps at one stage of life can become the dose that backfires when sleep is fragmented, body temperature swings more easily, and recovery is less predictable.
The issue is repeated maximum-effort work, especially stacked across the week. I see this often with women doing daily bootcamps, back-to-back sprint classes, or finishing every conditioning block at a 9 or 10 out of 10. They are disciplined, but their bodies are giving clear feedback. Hotter workouts. More night waking. Heavier fatigue the next day. A session that looks productive on paper can still be the wrong fit physiologically.
Menopause changes thermoregulation, and intense intervals produce a lot of heat quickly. If you already run hot, a workout built around all-out efforts can tip you from challenged into symptomatic. That does not always show up during the workout itself. Sometimes it shows up later as a poor night of sleep, an earlier hot flash, or a day where your legs feel flat and your patience is gone.
Recovery capacity also becomes less forgiving. High-intensity intervals raise stress hormones and create a larger recovery demand than moderate conditioning. Used once or twice a week, that can be a useful training tool. Used at maximum effort four, five, or six times a week, it often turns into a symptom amplifier rather than a fitness strategy.
The trade-off matters. HIIT can improve conditioning and insulin sensitivity. Too much maximum-effort HIIT can leave you exhausted, overheated, and inconsistent for the rest of the week. For many menopausal women, consistency beats hero workouts.
A simple test works well here. After a hard session, you should be able to recover well enough to sleep reasonably, function normally the next day, and train again without dragging soreness and irritability into every other workout. If HIIT repeatedly steals from tomorrow, the intensity, frequency, or format needs to change.
How to keep the benefit without the backlash
Most women do better with intervals that are hard but not all-out. Machine-based intervals often work better than floor-based circuits because they let you raise effort without adding as much impact, heat buildup, or frantic pacing.
Lower the effort ceiling: Aim for challenging repeats, not maximum effort every round.
Use fewer hard sessions: One to two interval sessions per week is often enough when symptoms are active.
Extend recovery periods: Longer easy intervals can keep body temperature and symptom flare-ups more manageable.
Choose lower-impact options: Bike, rower, elliptical, or incline walking usually have a better risk-reward ratio than repeated burpees or jump sprints.
Track your own triggers in Lila: Look for patterns between interval days and hot flashes, night sweats, poor sleep, or next-day irritability.
The goal is not to avoid intensity forever. The goal is to use it precisely, in a way your body can recover from.
6. Twisting and Rotational Exercises with Heavy Load
Weighted Russian twists, heavy landmine rotations, aggressive medicine-ball twisting, and fast rotational carries are common in group fitness. They’re usually sold as “functional core” work. During menopause, they can become an easy way to irritate the spine and pelvic floor without delivering much unique benefit.
This category matters even more if you have osteopenia, osteoporosis, prior back pain, or a history of disc irritation. Loaded twisting combines force, speed, and pressure, which is a poor combination when spinal tissues are less tolerant.
The problem with loaded rotation
Rotation itself isn’t the enemy. The issue is rotation under heavy load, especially when the movement is fast and the trunk isn’t controlling well. Women often feel this as a sharp low-back pinch during the workout or a dull ache that appears later when they sit, sleep, or bend.
Russian twists are a classic example. The exercise looks simple, but many people collapse through the lumbar spine, grip through the hip flexors, and whip side to side using momentum. That’s not high-quality core training. It’s repeated spinal motion under fatigue.
If you want a stronger waist and a steadier trunk, train resistance to rotation before adding more rotation.
A smarter swap is anti-rotation work. Pallof presses, dead bug variations, offset carries, and side planks train the torso to stay organized while the limbs move. Single-arm rows, split squats, and single-leg deadlifts also build the kind of real-world rotational control many women need.
Use less load or no load: Bodyweight rotation may be plenty if you tolerate it well.
Slow the speed down: Momentum hides poor mechanics.
Prioritize stability first: If anti-rotation drills feel hard, loaded twisting probably isn’t where you should start.
7. Excessive High-Impact Cardio on Hard Surfaces
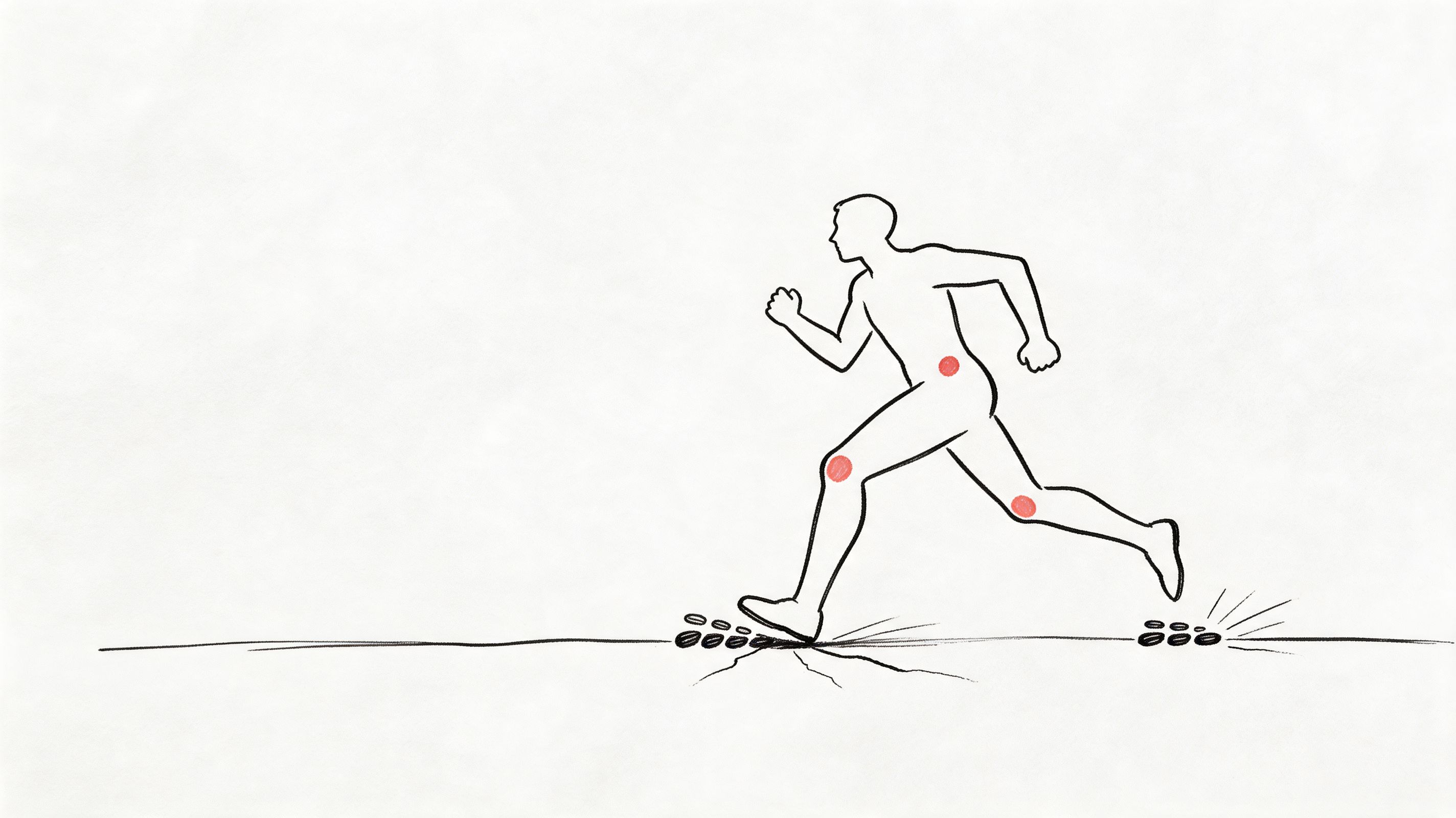
There’s a difference between enjoying an occasional run and relying on pounding pavement or treadmill mileage as your main form of cardio week after week. Excessive high-impact cardio on hard surfaces can become one of the least forgiving exercise patterns during menopause.
That’s especially true if your body is already giving warning signs. Sore feet when you get out of bed. Knees that ache going downstairs. Hips that tighten after workouts. A pelvic floor that feels heavy or irritated after runs. Those signals matter.
Why hard surfaces change the equation
Concrete and repetitive treadmill sessions can create cumulative stress through the ankles, knees, hips, and lower back. Add menopause-related changes in bone density, cartilage tolerance, and recovery, and the body may stop bouncing back between sessions the way it used to.
This is one place where women often get stuck in a false choice: run as usual or stop moving. There’s a much better middle ground. Keep cardio, reduce pounding, and spread your stress across more than one mode.
Swimming, cycling, rowing, elliptical training, and brisk walking are all strategic options. They support fitness without asking your joints to absorb the same repetitive impact. If you still want to run, use softer surfaces, shorten sessions, and build lower-body strength so impact is shared by stronger muscles rather than irritated joints.
What works better in practice
A woman who jogs daily on pavement may feel dramatically better with two shorter outdoor runs on a rubberized track, two cycling sessions, and two strength days. Her fitness doesn’t disappear. It often improves because she can finally recover.
Rotate your cardio modes: Don’t make every conditioning day a running day.
Use softer terrain when possible: Grass, trails, and tracks are often kinder than concrete.
Strength-train your shock absorbers: Glutes, calves, hamstrings, and trunk stability all help reduce impact stress.
Pay attention to delayed symptoms: Joint pain that shows up later still counts as exercise feedback.
7 Exercises to Avoid During Menopause: Quick Comparison
Exercise / Activity | Implementation Complexity 🔄 | Resource Requirements ⚡ | Expected Outcomes 📊 | Ideal Use Cases 💡 | Key Advantages ⭐ |
|---|---|---|---|---|---|
High-Impact Plyometric Exercises (Jump Squats, Box Jumps, Burpees) | Moderate, requires landing technique and impact tolerance | Low equipment; needs clear space, sturdy surfaces, good footwear | Rapid power and cardio gains; high joint & pelvic‑floor stress; may trigger hot flashes | Supervised athletic training only; otherwise swap for low‑impact cardio or resistance work | Time‑efficient power and cardio improvements |
Heavy Overhead Weightlifting Without Proper Support | High, advanced technique, core stability and mobility required | Barbell/rack, spotting/coaching, progressive loading and recovery | Strong upper‑body and core strength potential; increased fracture, spinal and pelvic‑floor risk | Experienced lifters with expert coaching; use supported alternatives for menopausal women | Builds upper‑body strength and functional capacity |
Intense Long‑Distance Running (Marathon Training) | Moderate, requires structured progressive plan and high mileage | Very time‑intensive (hours/week), quality footwear, recovery resources | Excellent endurance but sustained heat, cumulative joint/pelvic‑floor stress and cortisol elevation | Seasoned runners who tolerate volume; otherwise prefer shorter moderate sessions or cross‑training | High cardiovascular endurance and mental resilience |
Intense Core Work with Heavy Intra‑Abdominal Pressure (Heavy Crunches, Sit‑ups, Exhaustive Planks) | Low–Moderate, familiar techniques but high intra‑abdominal load to manage | Minimal equipment; may need pelvic‑floor physio guidance | Direct rectus abdominis strengthening; elevates intra‑abdominal pressure → worsened incontinence/prolapse risk | Avoid if pelvic‑floor or lumbar issues; use pelvic‑safe core patterns and guided rehab | Direct core targeting; easy to scale |
High‑Intensity Interval Training (HIIT) at Maximum Effort Frequency | Moderate, programmable but requires strict recovery and intensity control | Low equipment; time‑efficient but high recovery demand | Fast fitness gains; frequent max efforts raise cortisol, trigger hot flashes and disrupt sleep | Short, limited sessions (1–2/wk) with rest days; replace excess with moderate cardio | Highly time‑efficient conditioning |
Twisting & Rotational Exercises with Heavy Load (Weighted Russian Twists, Landmine Rotations) | High, needs controlled rotation technique and spinal stability | Weights/landmine, coaching recommended for spinal safety | Improves oblique strength but increases lumbar shear and pelvic‑floor pressure | Light, controlled rotation or anti‑rotation alternatives; consult PT if spine issues exist | Trains rotational strength when performed safely |
Excessive High‑Impact Cardio on Hard Surfaces (Pounding Pavement/Treadmill) | Low, easy to perform but requires load management | Time commitment, durable footwear, access to varied surfaces for modification | Strong cardiovascular benefits; cumulative joint wear, pelvic‑floor fatigue, and hot‑flash risk | Prefer low‑impact modalities (cycling, swimming, elliptical) or reduced frequency/duration | Accessible cardio with minimal skill needed |
Your Personalized Path to Menopause Fitness
The biggest mistake I see is treating menopause like a motivation problem when it’s often a programming problem. Many women are still working hard. They’re just using workouts that don’t match the body changes happening underneath the surface. That’s why lists of exercises to avoid during menopause matter only if they lead to better replacements, better timing, and better symptom awareness.
You don’t need to fear exercise. You do need to stop assuming that the hardest option is the most effective one. High-impact work, max-effort intervals, heavy unsupported overhead lifting, repeated spinal flexion, and loaded twisting all have a place in some training histories, but they’re not automatic wins during menopause. If they worsen hot flashes, joint pain, sleep, pelvic floor symptoms, or back pain, they’re costing more than they’re giving.
The better model is simple. Keep the intent, change the method. If you want intensity, use cycling, rowing, or brisk incline walking instead of endless jumping. If you want strength, use controlled resistance training with clear technique instead of chasing numbers your body can’t support well right now. If you want a stronger core, choose breathing-based stability work instead of ab burnout.
There’s also an important gap in the conversation: adaptation timing. We still don’t have a clear recovery and progression timeline that tells every woman exactly when she can safely reintroduce more impact or intensity. That means your own data matters. Symptom tracking is not overthinking. It’s how you find patterns between a workout and what happens later that day, that night, and the next morning.
That’s where a tool like Lila becomes useful. Instead of guessing whether HIIT is worsening your night sweats or whether pavement running is driving your knee pain, you can log the session, track the symptom pattern, and make changes based on what your body is reporting. That’s far more practical than following generic internet rules.
Sustainable menopause fitness usually looks less dramatic than the programs marketed to you. It’s often moderate cardio, strength training, mobility, balance work, and enough recovery to let those sessions help instead of hurt. That approach can still support bone health, mood, metabolic health, and confidence. It just does it with fewer flare-ups.
If you want a simple place to start, build around low-impact strength and cardio and explore resources like Zing Coach low impact exercises for ideas that feel athletic without being punishing. Then let your own symptom trends guide what you keep, modify, and drop.
If you want a more personalized way to connect your workouts with hot flashes, sleep, energy, mood, and recovery, Lila can help you do that in one place. The app lets you track symptoms and daily habits, then turn that information into a plan that fits your stage of perimenopause or menopause, so you can train with more confidence and less trial and error.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.