Perimenopause Joint Pain Relief Strategies That Work
Discover why perimenopause joint pain occurs and get evidence-based lifestyle, exercise, and medication tips to ease discomfort. Track progress with Lila.
More than 7 in 10 perimenopausal women experience musculoskeletal pain according to a meta-analysis, and the odds are 1.63 times higher than in premenopause** (PMC). That changes the way many women hear their own symptoms. Sudden knee stiffness, aching fingers, sore hips, or a back that feels strangely older than the rest of you may not be random.
For many women, perimenopause joint pain begins subtly. You wake up and your feet feel stiff on the floor. You grip a coffee mug and notice your hand hurts. You stand after sitting for a while and your knees complain. It can feel unsettling because the pain often moves around. One week it's your shoulders. The next, your wrists or hips.
That pattern creates confusion. Is it arthritis? Is it overuse? Is it just aging? Sometimes it is one of those things. Sometimes it isn't.
Perimenopause can affect joints through hormonal shifts that ripple through cartilage, muscles, tendons, bone, sleep, and inflammation. The result can be real pain without a simple blood test to confirm it. That doesn't mean it's imaginary. It means the body is changing in a way many women were never taught to expect.
Introduction to perimenopause joint pain
A lot of women expect hot flashes. Fewer expect their joints to become the loudest symptom in the room.
Perimenopause joint pain often shows up as stiffness first. A woman in her mid-40s might notice that stairs feel different, rings feel tighter on sore fingers, or getting up from the couch takes a second longer than it used to. She may still be exercising, working, and managing a full life, but her body starts sending mixed messages.
That mismatch is part of what makes this symptom so frustrating. You may look healthy, but your knees, hands, shoulders, or lower back feel off. The pain may migrate. It may flare before a period, after poor sleep, or during especially stressful weeks. Some days feel normal. Other days don't.
Perimenopause joint pain also gets dismissed too easily. Women are often told they're just tired, just stressed, or just getting older. Aging does affect joints, but midlife hormone shifts can change how your body handles inflammation, joint lubrication, muscle support, and recovery. That makes aches more likely and often more noticeable.
Perimenopausal joint pain is common, but common doesn't mean you have to ignore it.
A useful starting point is this: if your joint pain appeared alongside cycle changes, sleep problems, mood shifts, or other perimenopausal symptoms, it's worth looking at the whole picture rather than treating each ache as a separate mystery.
Understanding why joint pain occurs during perimenopause
Joint pain in perimenopause isn't caused by one single switch flipping off. Several body systems change at the same time, and joints sit right in the middle of that conversation.
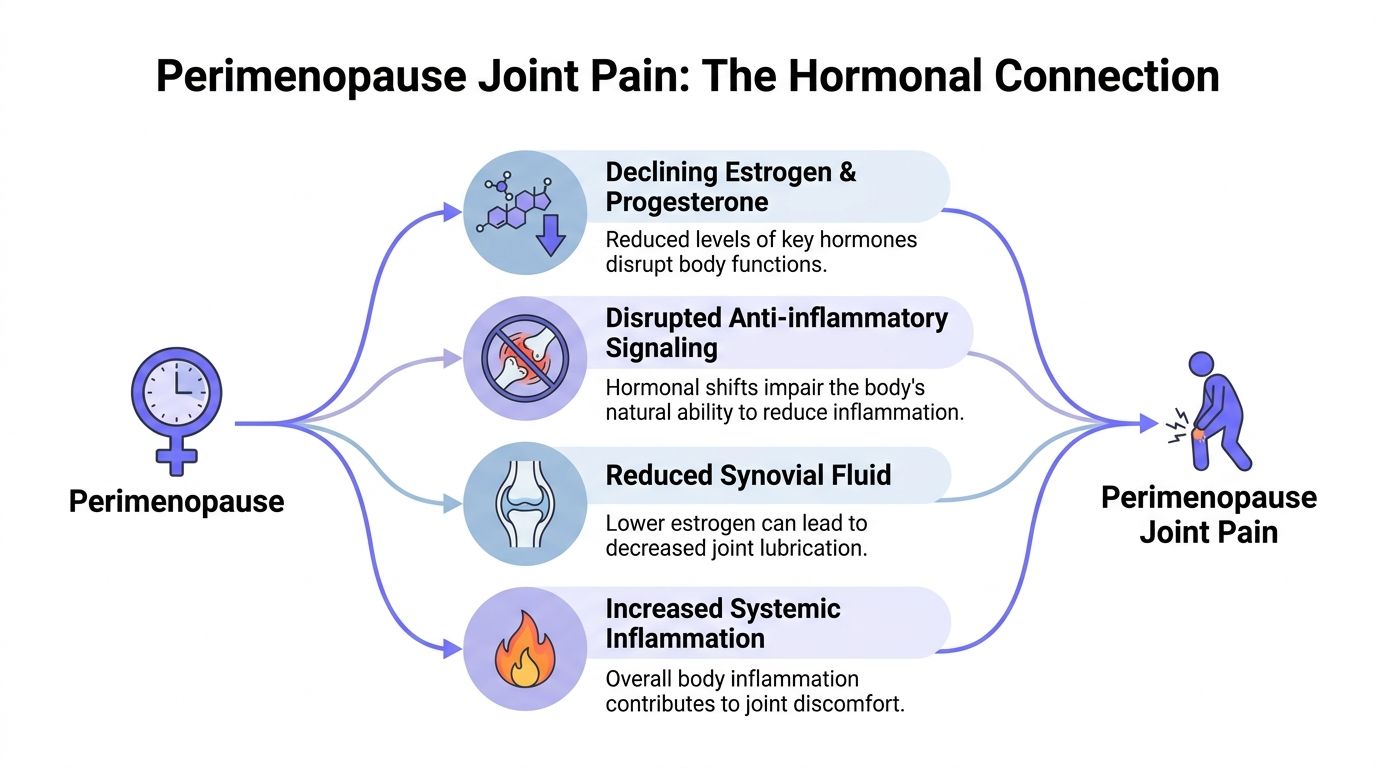
Hormones affect far more than periods
Estrogen receptors are present in bone, cartilage, synovium, muscles, and tendons, which helps explain why hormone decline can trigger body-wide changes rather than pain in just one spot. One source summarizes the chain clearly: hormone decline can mean 50% less joint lubrication, 1 to 2% annual muscle loss, and 1 to 3% yearly bone density drop, all contributing to migratory joint pain (Natural Cycles).
If that sounds abstract, think of a joint like a well-fitted door hinge. It works best when the moving parts are supported, cushioned, and lightly lubricated. During perimenopause, the body may provide less of that internal support. The hinge still moves, but it does so with more friction and less stability.
Progesterone shifts can add to the problem. While estrogen gets most of the attention, progesterone also plays a role in inflammation and tissue support. When both hormones become erratic, some women notice more stiffness, more soreness after activity, and slower recovery.
Why the pain can move around
Classic wear-and-tear pain often stays in one familiar place. Perimenopause joint pain is often less tidy.
You may feel:
Hands that ache in the morning and then loosen up later
Knees that hurt after sitting even if you didn't injure them
Shoulders or hips that flare without a clear trigger
Low back discomfort during poor sleep weeks or cycle shifts
That migratory pattern happens because the hormone changes aren't limited to one joint. They influence tissues across the musculoskeletal system.
Inflammation, lubrication, and support all matter
Three processes often overlap:
Process | What changes | What you may feel |
|---|---|---|
Inflammation | Lower hormone support can make inflammatory signaling harder to regulate | Achiness, puffiness, general soreness |
Lubrication | Less synovial support can increase friction in moving joints | Stiffness after rest, creaky movement |
Muscle support | Declining muscle mass can reduce joint stability | More strain with stairs, lifting, walking, or repetitive tasks |
Poor sleep can make all of this feel sharper. So can stress, because stress affects recovery, pain sensitivity, and muscle tension. That's one reason some women say their joints hurt more after several rough nights than after a workout.
Practical rule: If your pain feels widespread, variable, and oddly connected to sleep, stress, or cycle changes, don't assume you're imagining it. That's a pattern worth tracking.
It's not just aging
Women often blame these symptoms on age because that's the most familiar explanation. But timing matters. If joint pain appears during the years when periods change, recovery slows, and other hormonal symptoms show up, hormones may be part of the reason.
That doesn't mean every ache is hormonal. It means hormones can lower the body's margin for comfort. A workout that once felt fine now leaves you sore for days. A desk setup you tolerated for years suddenly irritates your neck and shoulders. Existing arthritis may also feel more noticeable when hormonal support drops.
The key idea is simple. Perimenopause joint pain is usually a whole-body issue with local symptoms. Your knee may hurt, but the story may involve sleep, hormones, muscle support, and inflammation all at once.
Differentiating joint pain from other conditions
Not all midlife joint pain is perimenopause joint pain. That's why a careful rule-out process matters.
One of the hardest parts is that no gold-standard test exists, even though more than 40% of women report musculoskeletal pain before and during the menopause transition. Guidance on how to tell hormone-related pain from treatable arthritic conditions is still thin (The Origin Way).
Start with the pattern, not the label
Before assuming anything, look at how the pain behaves.
Ask yourself:
Where is it? Does it move between joints, or stay in one place?
What time of day is it worse? First thing in the morning, after sitting, or after activity?
Is there swelling, warmth, or redness?
Did it follow an injury or a new sport, workout, or repetitive task?
Did it appear around the same time as cycle changes, hot flashes, mood shifts, or sleep disruption?
Hormone-related aches often feel broad, bilateral, or migratory. In contrast, an injury usually has a clearer starting point. Osteoarthritis often feels more mechanical and location-specific. Inflammatory arthritis may come with visible swelling, prolonged stiffness, or other systemic signs.
A simple discussion guide for your appointment
Bring notes instead of relying on memory. A clinician can do much more with patterns than with a vague, "Everything hurts."
This can help:
Map the joints involved by writing down hands, knees, hips, shoulders, feet, or back
Track associated symptoms such as poor sleep, mood changes, irregular periods, or hot flashes
Note what changes the pain including rest, walking, strength work, stress, or weather
Record red flags such as one-sided swelling, fever, sudden severe pain, or loss of function
If you're still sorting out whether discomfort is coming from the joint itself or the surrounding tissue, this guide on differentiating joint pain or muscle pain can make your notes more precise.
You may also find it helpful to compare symptoms with common midlife muscle complaints in this internal guide on https://getlila.com/blog/perimenopause-muscle-pain.
When labs or referrals make sense
A clinician may consider basic inflammation markers such as CRP or ESR, and in some cases imaging or a rheumatology referral. Those steps matter more when symptoms don't fit the usual hormone-related pattern.
A referral deserves stronger consideration if you have:
Persistent swelling
A hot or visibly inflamed joint
Pain focused in one area that keeps worsening
Symptoms that interfere with gripping, walking, or climbing despite rest
A personal or family history of autoimmune disease
Midlife hormone changes can coexist with osteoarthritis, rheumatoid arthritis, lupus, tendon problems, or old injuries. The goal isn't to guess the cause. It's to narrow it carefully.
That distinction matters because treatment changes depending on the cause. A hormone-related pattern may respond to sleep support, exercise progression, and medical menopause care. A meniscus injury, inflammatory arthritis, or gout needs a different path.
Managing joint pain with lifestyle and exercise
Joint pain often improves when you reduce irritation and rebuild support at the same time.
A 2024 survey found that over 32% of women report joint or muscle pain during the menopause transition, and more than 40% face stiffness linked to estrogen decline (Harvard Health). That doesn't point to one miracle fix. It points to the need for targeted daily habits.
The lifestyle basics that make movement easier
Start with the inputs that shape recovery.
Sleep protection matters because poor sleep amplifies pain sensitivity. Keep wake time consistent and lower stimulation before bed.
Anti-inflammatory eating patterns can help some women notice fewer flares. Many do well by emphasizing omega-3-rich foods, fiber-rich plants, adequate protein, and steady meals rather than long stretches without eating.
Stress regulation matters because stress tightens muscles and worsens recovery. Short walks, breathing drills, or a brief stretch routine can lower the "braced" feeling many women carry all day.
Pacing beats boom-and-bust exercise. If you push hard on a good day and crash for two days after, your plan needs a smaller starting point.
A simple three-week exercise build
The goal isn't to punish painful joints. It's to help them feel safer and more supported.
Week one
Focus on daily motion and gentle strength.
Walk or cycle gently on most days if tolerated
Do short mobility work for hips, ankles, shoulders, and wrists
Add two strength sessions using body weight or light resistance
Keep sessions short so your body finishes feeling better, not worse
A practical place to start is with controlled resistance band mobility exercises that move stiff joints without high impact.
Week two
Begin adding structure.
Try:
Three resistance sessions focused on major muscle groups
Two lower-impact recovery days such as swimming, easy yoga, or a long walk
Daily range-of-motion work for the joints that stiffen most after rest
Sample strength choices:
Sit-to-stands or squats to a chair
Glute bridges
Rows with a band
Wall push-ups
Calf raises
Dead bugs or other gentle core work
Week three
Build consistency before intensity.
Day | Focus | Example |
|---|---|---|
Monday | Strength | Lower body and core |
Tuesday | Mobility | Gentle yoga, walking |
Wednesday | Strength | Upper body and posture work |
Thursday | Recovery | Swim, stretch, easy walk |
Friday | Strength | Full body session |
Saturday | Movement | Light hike or long walk |
Sunday | Reset | Mobility and rest |
For more ideas, this internal guide to menopause-friendly movement can help: https://getlila.com/blog/best-exercises-for-menopause
How to know if you're doing the right amount
The best exercise plan for perimenopause joint pain usually feels almost too easy at first.
Watch for these responses:
Good sign. Mild soreness that settles and better stiffness after movement
Yellow flag. Pain that lingers into the next day and changes how you walk or use your hands
Red flag. Sharp pain, swelling, or symptoms that keep escalating
Movement should build trust with your joints. If every session feels like a threat, scale down the load, shorten the range, or reduce the duration.
A common mistake is skipping strength work because the body feels fragile. In reality, stronger muscles often act like shock absorbers. They take pressure off joints and improve everyday tasks such as climbing stairs, carrying groceries, or sitting at a desk without bracing.
Medical treatments and supplements for joint pain
Lifestyle work matters, but some women need additional help. That's especially true when pain affects sleep, activity, work, or mood.
The medical options range from symptom relief to hormone support. The right choice depends on your symptom pattern, overall health history, and whether joint pain is showing up alongside other menopausal symptoms.
Symptom relief options
Some women start with local pain control.
Option | Potential role | Main trade-off |
|---|---|---|
Topical anti-inflammatory gel | Useful for a specific sore joint such as a knee or hand | Relief is often local rather than whole-body |
Oral anti-inflammatory medication | Can help during flares | May not suit everyone, especially with stomach, kidney, or blood pressure concerns |
Physical therapy | Helps when weakness, mechanics, or posture are contributing | Requires consistency and a tailored plan |
These tools can reduce pain enough to help you keep moving, which often matters as much as the medication itself.
When hormone therapy enters the conversation
If joint pain sits alongside hot flashes, sleep disruption, mood changes, or cycle instability, menopause hormone therapy may be worth discussing.
One verified summary reports that combined transdermal estradiol at 0.5 to 1 mg and micronized progesterone at 100 to 200 mg yields 50 to 70% relief in perimenopausal joint pain, outperforming exercise alone in randomized trials (Mass General Brigham).
That doesn't mean hormone therapy is right for every woman. It does mean joint pain may improve when the hormonal driver is addressed directly.
How to think about the options
Use a decision lens rather than looking for one universal answer.
If your pain is mild and intermittent
You may do well with:
activity modification
progressive strength work
sleep support
occasional topical relief
If your pain is broad and tied to other perimenopause symptoms
Ask your clinician whether hormone treatment belongs in the conversation, especially if:
sleep has deteriorated
periods have become irregular
you have hot flashes or night sweats
the pain feels migratory rather than injury-based
If the pain is focal, swollen, or inflammatory
The priority shifts. A careful evaluation for arthritis, tendon injury, or another condition comes first.
Joint pain treatment works best when it matches the pattern. Broad hormonal pain, a swollen knuckle, and a torn tendon don't need the same solution.
Supplements worth discussing with a clinician
A few categories come up often:
Omega-3s are commonly used when inflammation seems to be part of the picture
Vitamin D may be discussed in the context of bone health
Other supplements sometimes appear in marketing, but evidence and quality can be inconsistent
It's smart to bring every supplement to your clinician or pharmacist, especially if you take other medications. "Natural" doesn't always mean low-risk, and it doesn't guarantee that a product contains what the label promises.
A productive visit often starts with a short list: what you've tried, how your pain behaves, what other symptoms travel with it, and what outcomes matter most to you. For some women, success means walking without stiffness. For others, it's sleeping through the night or getting back to tennis, gardening, lifting, or typing without dread.
Tracking progress with the Lila app
Symptoms are easier to treat when you can see their pattern.
Perimenopause joint pain is hard to describe from memory because it often shifts by day, body part, sleep quality, and cycle timing. A woman may say, "My joints hurt all the time," yet the pain's pattern is often more specific. Worse after poor sleep. Better after light movement. Strongest in the hands before a period. Quieter during lower-stress weeks.
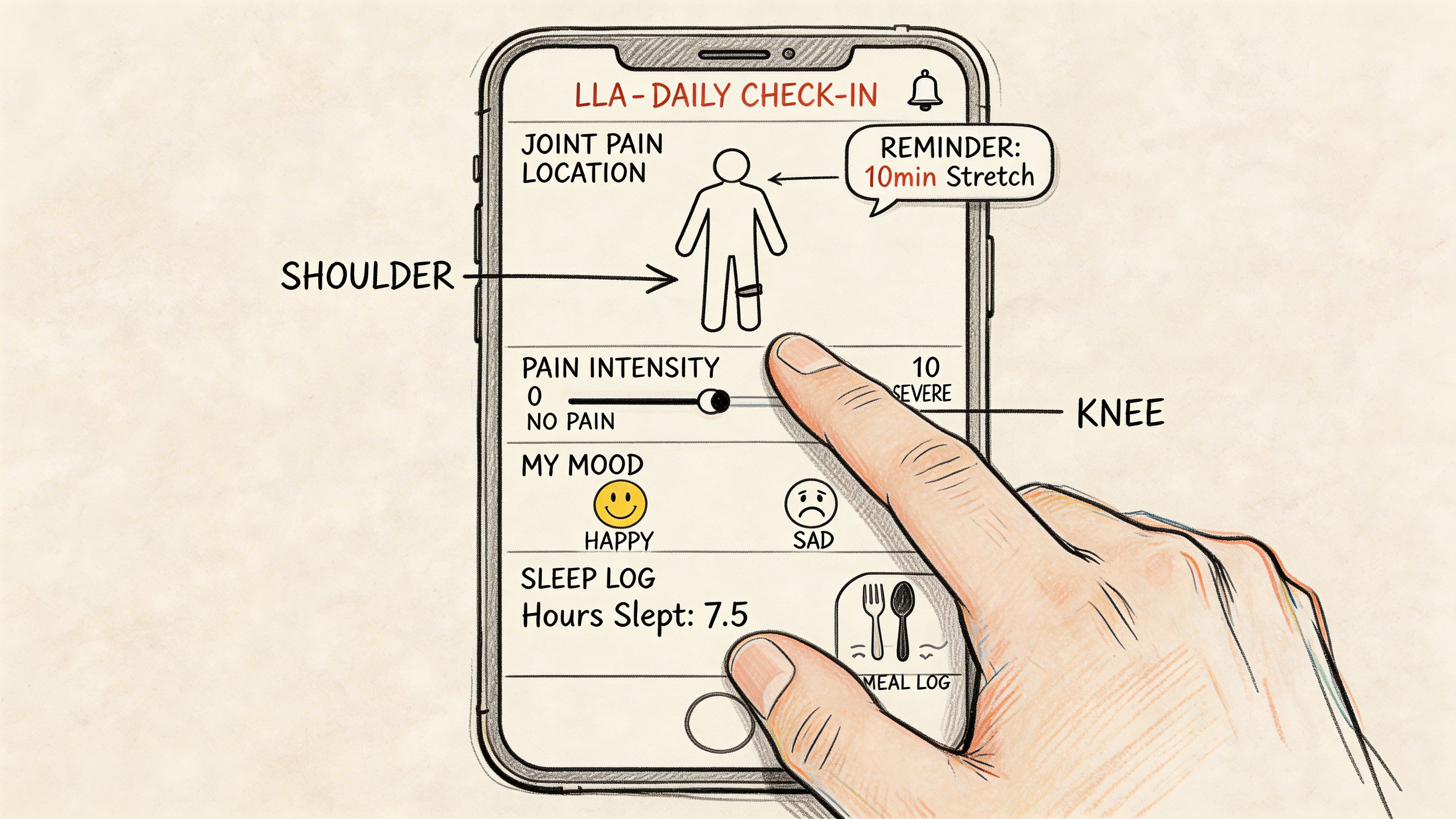
What to log each day
A useful tracking system doesn't need to be complicated. It needs to be consistent.
Record:
Pain location such as hands, hips, knees, shoulders, feet, or back
Pain intensity in your own words or a simple personal scale
Timing including morning stiffness, post-exercise flares, or evening aching
Related symptoms like poor sleep, mood shifts, bloating, or hot flashes
What helped including walking, stretching, heat, rest, or medication
Lila is one option for this kind of structured symptom tracking. It lets users log symptoms, sleep, mood, meals, energy, and cycles in one place, which can help reveal whether joint pain flares cluster with other perimenopausal changes. This overview of a https://getlila.com/blog/menopause-symptom-tracker-app shows what that kind of daily log can look like.
Why tracking changes decision-making
Patterns turn vague discomfort into actionable information.
Instead of saying:
"My knees are bad lately"
You can say:
"My knee and hand stiffness are worst after poor sleep and improve after gentle strength work"
"My shoulder pain shifts with cycle changes and stress-heavy weeks"
"My hips flare after long sitting, not after walking"
That makes clinician visits more useful. It also helps you test interventions one at a time.
A better way to adjust your plan
Try this simple review each week:
Question | Why it matters |
|---|---|
Where did pain show up most? | Helps distinguish widespread versus focal patterns |
What happened before flare days? | Can reveal links with sleep, stress, food, or inactivity |
What consistently helped? | Points toward routines worth keeping |
What made symptoms worse? | Shows where to scale back or ask for help |
Small daily observations can reveal trends that memory misses.
A log also prevents overcorrecting. If one rough day follows a strong week, you don't need to scrap the whole plan. You need to check what changed. Tracking gives you that context.
Real-life joint pain management examples
No two women experience perimenopause joint pain in exactly the same way. The pattern changes with work, sleep, old injuries, and activity level. These examples show how the same principles can be adapted without pretending there's one perfect formula.
The runner with stiff knees
A woman in her mid-40s noticed that her knees felt stiff when she started running, but loosened after a warm-up. She also had irregular periods and more broken sleep than usual.
Her first move wasn't to quit exercise. She reduced high-impact mileage for a few weeks, added lower-body strength work, and started a short mobility routine before runs. She also paid attention to whether bad nights led to worse morning stiffness.
The key shift was seeing that her knees didn't hurt in isolation. Sleep and recovery were part of the picture. Once she treated the whole pattern instead of chasing the knee alone, movement became more predictable.
The desk worker with wrist and shoulder pain
A woman around age 50 developed aching wrists and shoulder tightness during long computer days. She worried it was early arthritis because typing and gripping felt harder by afternoon.
Her clinician looked for red flags and didn't find obvious signs of an inflammatory joint condition. She then adjusted her workstation, took brief movement breaks, and began upper-back and shoulder strengthening. She also noticed that symptoms flared during stressful weeks and around other menopause symptoms.
What helped most was combining mechanical fixes with body-wide awareness. Better posture alone wasn't enough. Better recovery alone wasn't enough. Together, they gave her a clearer baseline.
The gardener with hip discomfort
A woman in her late 40s loved gardening but found that prolonged crouching and lifting left one hip angry for days. Because the pain was more localized, she needed to rule out a structural problem rather than assuming it was hormonal.
Her care plan centered on evaluation first, then a gradual return to activity, glute strengthening, and pacing heavy yard work into shorter blocks. She kept notes on what positions triggered the pain most. That helped her separate task-related strain from the more general whole-body stiffness she noticed during hormonally rough weeks.
Relief often comes from combining the right diagnosis with the right habit changes, not from forcing one explanation to fit every symptom.
These examples matter because they show what real progress usually looks like. Not instant, not linear, and not identical from person to person. The win is learning your pattern well enough to make smarter choices week by week.
Conclusion and next steps
Perimenopause joint pain can feel random, but it usually isn't. Hormone shifts can affect inflammation, lubrication, muscle support, and recovery across the whole body. That's why the pain may move, flare unpredictably, and overlap with sleep changes, mood shifts, or cycle changes.
A practical next-step checklist looks like this:
Track symptoms for two weeks so you can spot patterns instead of relying on memory
Rule out other conditions if pain is swollen, one-sided, worsening, or clearly inflammatory
Start a three-week movement plan built around gentle mobility, progressive strength, and recovery
Review medical options with a clinician if pain is broad, persistent, or tied to other menopausal symptoms
Adjust based on trends rather than reacting to one bad day
You don't need to white-knuckle your way through this stage of life. Joint comfort often improves when the plan matches the cause. The more clearly you can see your own pattern, the easier it becomes to choose the next right step.
If you want a simple way to track symptoms, meals, sleep, mood, and cycle changes in one place, Lila offers an AI-guided approach that can help you connect daily habits with how you feel and build a more personalized plan for perimenopause symptoms.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.