Joint Pain in Menopause Treatment: Your Guide
Struggling with aches? Discover effective joint pain in menopause treatment options. Explore therapies & lifestyle changes to manage your symptoms.
You wake up, swing your legs out of bed, and your body doesn't quite follow your plans. Your fingers feel stiff around the coffee mug. Your knees protest when you stand. Your hips seem older than they did a month ago. A lot of women in their 40s and 50s have this exact moment and wonder the same thing: Why do my joints suddenly hurt when I haven't done anything unusual?
That question matters because this kind of pain often gets brushed off as "just aging." Sometimes it is wear and tear. But sometimes it's part of the menopausal transition, when hormone changes affect far more than periods and hot flashes. Joints, muscles, sleep, mood, and energy can all shift together.
The good news is that joint pain during menopause is real, common, and treatable. The most effective plan usually isn't a single fix. It tends to be a combination of medical guidance, targeted exercise, daily habits, and careful symptom tracking so you can tell what's helping.
Waking Up to Aches You Can't Explain
It often starts subtly. Maybe your ankles feel tight when you walk downstairs in the morning. Maybe your shoulders ache after a normal workday at the computer. Maybe your hands feel puffy and awkward when you button a shirt, even though nothing looks obviously wrong.

For many women, the frustrating part isn't just the discomfort. It's the uncertainty. You may still be active. You may not have had an injury. You may even have normal lab work and still feel stiff, sore, or creaky in ways that don't make sense.
That mismatch can be unsettling. When pain appears without a clear cause, people often doubt themselves. They wonder if they're overreacting. They push through. They wait for it to pass.
Joint pain in menopause treatment starts with one important truth: if your body feels different, you're not imagining it.
Morning stiffness, sore hips after sitting, cranky knees during a walk, or aching shoulders at night can all fit the bigger picture of menopause-related musculoskeletal change. The symptom may show up before you connect it to hormones, especially if you don't have dramatic hot flashes.
A more helpful way to think about it is this: your body is adapting to a major internal shift, and your joints are part of that story. Once you understand why it's happening, treatment feels much less random. You can make better decisions about hormone therapy, pain relief, strength training, sleep, and how to build a routine you can stick with.
Why Your Joints Hurt During Menopause
Joint pain during menopause usually has more than one cause. Hormone shifts are often part of it, but they interact with sleep, muscle strength, stress, past injuries, and the normal wear that builds up over time. That is why relief often comes from a plan, not a single fix.
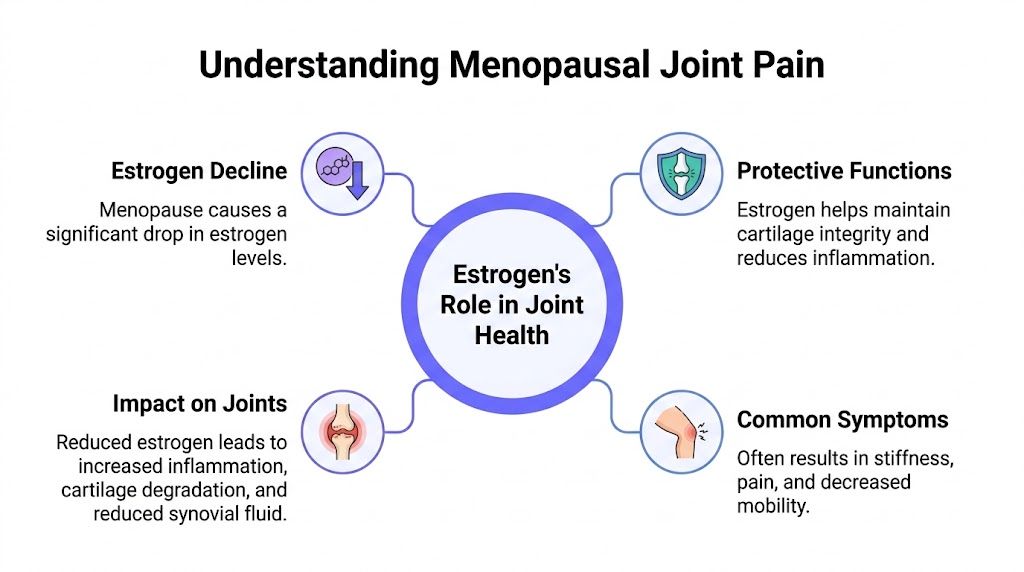
Estrogen helps maintain joint tissue
Estrogen affects far more than periods and hot flashes. It also helps regulate inflammation, supports cartilage, and influences how muscles and connective tissue recover after everyday movement.
As estrogen levels fall, the whole system can feel less forgiving. A staircase that used to feel routine may leave your knees irritated. Sitting through a meeting may make your hips stiff. Sleeping on one side may leave a shoulder sore in the morning. The joint has not necessarily been injured. It may be responding differently to the same load.
Consequently, joint pain in menopause treatment often needs to look beyond one painful spot. For some women, the problem is not a single joint. It is a body adjusting to lower estrogen, poorer sleep, and changing muscle support all at once.
If you want a clearer picture of where hormone therapy fits into that bigger picture, this guide on what hormone therapy for menopause can and cannot help with explains the role of treatment in practical terms.
Menopause can change the pattern of pain
Menopause-related joint pain does not always behave like a classic injury. It may move around. It may flare after inactivity, then ease once you get going. It may feel worse after a bad night of sleep or during a stressful week.
Common areas include the knees, hips, shoulders, hands, and feet. Some women notice a dull, widespread ache. Others feel a sharper pain in one area layered on top of general stiffness.
A broader pattern has shown up in population data. A 2024 AARP report on menopause joint pain notes that joint and muscle pain are common during menopause, and that osteoarthritis becomes more common and more severe after menopause.
The timing of the pain is a meaningful clue. If aches begin during perimenopause or after menopause, hormones may be contributing even when they are not the whole explanation.
Why this gets confusing fast
Several changes can stack together and blur the picture:
Hormone decline: less estrogen support for joint comfort and tissue maintenance
Muscle changes: weaker muscles around a joint can increase strain during normal movement
Sleep disruption: poor sleep can heighten pain sensitivity
Inflammation and stress: both can amplify soreness and stiffness
Midlife joint changes: old injuries, hypermobility, or early arthritis may become harder to ignore
This overlap is why two women can both say, "my joints hurt," and need different solutions. One may benefit most from better sleep and strength training. Another may need an arthritis evaluation. Another may find that treating hot flashes with hormone therapy indirectly improves pain by restoring sleep, while the hormone therapy itself offers only modest direct joint benefit.
That nuance helps you avoid oversimplified answers. It also points toward a more useful approach. Track when pain shows up, look for patterns, and combine medical guidance with daily habits that reduce strain and inflammation.
Exploring Medical Treatments for Joint Pain Relief
Medical care works best when you treat joint pain like a puzzle, not a single symptom. One piece may be hormone change. Another may be inflammation in a specific joint. A third may be poor sleep, reduced activity, or early arthritis. The goal is to match the treatment to the pattern.
Where hormone therapy fits
Hormone replacement therapy, also called menopause hormone therapy, often comes up early in this conversation because estrogen affects many tissues, including those involved in joint comfort. Some women do notice that aches improve after starting treatment.
The nuance matters. HRT is mainly prescribed for menopause symptoms such as hot flashes and night sweats. It is not usually prescribed for joint pain by itself. Mass General Brigham explains that menopause hormone therapy is not recommended solely for isolated joint pain, while also noting that some women may experience secondary relief, especially if better sleep and fewer vasomotor symptoms lower their overall pain burden. Their discussion of menopause, hormones, and musculoskeletal symptoms is summarized in this medical overview of menopause and joint pain.
A practical way to think about HRT is that it may help some women indirectly and sometimes directly, but it is not the main first-line treatment for every aching joint. If you are weighing the pros and cons, this guide to what hormone therapy for menopause is can help you prepare for a more informed conversation with your clinician.
Nonprescription pain relief
For short-term symptom control, over-the-counter treatment can make daily movement easier, which matters because stiff joints often feel worse when you avoid using them.
Common options include:
NSAIDs: medicines such as ibuprofen can reduce inflammation and pain
Acetaminophen: this can help pain, though it does not reduce inflammation the same way
Topical products: gels or creams may help when pain is limited to one area, such as a knee, hand, or shoulder
These tools are for symptom relief. They do not correct the hormone shift underneath menopause, but they can lower pain enough to help you keep walking, stretching, and sleeping more comfortably.
When one joint needs its own workup
Sometimes menopause is the backdrop, but the loudest problem is a single joint. A painful shoulder may be frozen shoulder. A swollen knee may be osteoarthritis. Hip pain may be coming from the joint, nearby tendons, or even the lower back.
That is why a focused medical evaluation can be so helpful. Depending on the pattern, your clinician may suggest physical therapy, imaging, or an injection for a clearly inflamed joint. Corticosteroid injections can help selected cases, but they are targeted tools, not a general treatment for all menopause-related aches.
If fatigue is showing up alongside pain, it can also be useful to look at broader contributors such as inflammation, diet, or other health issues. Some women seek outside education on help with joint pain and fatigue as they sort through possible causes with their clinician.
A good appointment often starts with a better question: "Does this seem mainly hormone-related, mainly joint-specific, or a mix of both?"
That wording helps you and your clinician build one plan from three angles. Medical treatment for symptoms. A check for joint conditions that need specific care. Daily tracking so you can see what changes occur after you start treatment.
Powerful Lifestyle Strategies to Soothe Aching Joints
The strongest long-term improvements usually come from what you do consistently, not what you do once. Lifestyle care doesn't mean settling for less effective treatment. In many cases, it's the foundation that makes everything else work better.
Build strength to protect your joints
When muscles around a joint get stronger, they help absorb force and stabilize movement. That can make walking, standing up, climbing stairs, and carrying groceries feel easier.
An orthopedic review notes that supervised resistance training can reduce joint compressive forces by 20 to 30%, and a progressive home-based routine done 2 to 3 times per week improved WOMAC pain scores by 25 to 40% over 12 weeks in menopausal women, according to this orthopedic perspective on menopause and joint pain.
You don't need to start with a hard-core gym plan. A smart beginner routine might include:
Chair squats or bodyweight squats: helpful for hips, thighs, and knees
Wall push-ups: easier on wrists and shoulders than floor push-ups
Rows with a resistance band: good for posture and upper back support
Step-ups on a low step: useful for leg strength and balance
Glute bridges: often helpful when hip or low back discomfort is part of the picture
Start slowly. Good form matters more than intensity.
Choose movement that calms, not punishes
A common mistake is stopping activity altogether. Rest has a place during flares, but too much inactivity tends to make joints stiffer.
Low-impact movement is often the sweet spot. Walking, swimming, gentle cycling, yoga, and mobility work can help keep joints moving without the pounding of high-impact workouts.
A simple rule works well: if an activity leaves you feeling looser afterward or only mildly sore the next day, it's probably within range. If it repeatedly causes a flare that lasts, it needs adjusting.
Practical rule: aim for regular movement you can repeat, not heroic workouts you dread.
If you're also dealing with fatigue, food sensitivity concerns, or inflammation-related symptoms, some women like to explore broader supportive resources such as this guide on help with joint pain and fatigue. It's not a substitute for medical care, but it can prompt useful questions about patterns, triggers, and overall symptom load.
Eat in a way that supports recovery
No single food cures menopausal joint pain. But eating patterns can affect inflammation, energy, sleep, and body comfort.
A practical anti-inflammatory style of eating usually emphasizes:
Protein at meals: supports muscle maintenance while you're building strength
Colorful produce: fruits and vegetables add fiber and compounds linked with overall health
Healthy fats: especially foods that naturally contain omega-3 fats
Steady hydration: joints and muscles tend to feel worse when you're underhydrated
Less ultra-processed food if it seems to worsen symptoms: some women notice more swelling or sluggishness when their diet gets highly refined
Some women also ask about supplements. The answer depends on the person, the diet, and any medical conditions. If you want a grounded overview, this article on the best menopause supplements can help you sort hype from reasonable options.
Here's a movement session you can follow along with when you want guided support:
▶ PlayDon't ignore sleep and stress
Pain and poor sleep often reinforce each other. If you sleep badly, pain feels sharper the next day. If you hurt more, you sleep worse the next night.
That means joint pain care isn't only about joints. Better sleep hygiene, a consistent bedtime, a cooler bedroom, and calming evening routines can all help lower the total symptom load. Some women also find that breathwork, mindfulness, or a warm bath reduces muscle guarding and makes sleep easier.
You don't need perfection. You need enough consistency for your body to start trusting the routine.
Your Daily Plan for Managing Menopause Joint Pain
When symptoms pile up, advice can feel abstract. A daily rhythm makes it easier to follow through. The goal isn't to do everything. It's to repeat a few useful things often enough that your joints get a fair chance to respond.
Morning reset
Start gently, especially if mornings are your stiffest time.
Try this sequence before the day gets busy:
Warm first: a shower, heating pad, or warm drink while you move a little
Loosen key joints: slow ankle circles, shoulder rolls, wrist mobility, and easy hip stretches
Wake up muscles: a short set of sit-to-stands or wall push-ups can help you feel less rusty
Take stock: notice where pain sits today and whether it's stiffness, swelling, or sharp pain
During the day
Long periods of sitting can make symptoms louder. Small movement breaks usually work better than waiting for one perfect workout.
A practical daytime approach:
After desk time: stand up and walk briefly
During errands: park a bit farther away if that feels manageable
At lunch or midafternoon: do a short walk or a few mobility drills
If one joint is irritated: use supportive footwear, adjust posture, or reduce repetitive strain
Here is a simple comparison table you can use as a quick reference.
Approach | Examples | Primary Goal | Key Consideration |
|---|---|---|---|
Medical support | Hormone therapy discussion, OTC pain relief, physical therapy referral | Reduce symptoms and rule out other causes | Best chosen with a clinician, especially if symptoms are new or severe |
Strength work | Squats, rows, bridges, resistance bands | Support joints with stronger muscles | Start with manageable loads and good form |
Low-impact movement | Walking, yoga, swimming, cycling | Maintain mobility and reduce stiffness | Consistency matters more than intensity |
Recovery habits | Sleep routine, heat, stress reduction | Lower pain sensitivity and improve recovery | Pain often improves when sleep improves |
Tracking | Daily symptom notes, activity log, meal and sleep patterns | Identify what helps and what flares symptoms | Patterns are easier to see when written down |
Evening wind-down
Evenings are a good time to reduce inflammation triggers and prepare for better sleep.
A calm routine might include a warm bath, light stretching, or a few minutes of breathwork. If a joint tends to ache after activity, this is also a good time to use doctor-approved pain relief strategies or gentle self-massage around the area.
The best plan is one you can still do on a tired Tuesday, not just on your most motivated day.
How Lila Helps You Track and Manage Your Plan
You wake up stiff, but by lunch your hands feel better. Two days later, your knees ache after a short walk that usually feels fine. Menopause joint pain often behaves like that. It shifts with sleep, stress, activity, and other symptoms, which makes it hard to tell what is effective.
A tracking tool helps turn a blurry picture into a clearer one. Instead of asking yourself, "Why do I hurt today?" you can start asking better questions. Did the flare follow a poor night of sleep? Did stiffness improve on days you did gentle strength work? Did pain rise during a week with more hot flashes, which may point back to the broader hormone shift rather than a single workout or food?
That kind of pattern-finding matters because menopause joint care usually works best as a plan, not a one-off fix. Medical treatment, movement, recovery, and symptom tracking fit together. If HRT is part of your discussion with a clinician, tracking can also help you separate its main role from its possible side benefits. HRT is primarily used for symptoms like hot flashes and night sweats. Some women also notice joint symptom improvement, as noted earlier, but it is not a guaranteed or stand-alone treatment for every type of joint pain.
What to track each day
Keep it simple enough that you will do it.
Pain details: which joint hurts, how strong the pain feels, and whether it is stiffness, soreness, or sharper pain
Morning function: how you feel getting out of bed, using stairs, opening jars, or starting your day
Sleep: hours slept, night waking, and whether you feel restored
Movement: walking, stretching, strength work, long sitting periods, or a more active-than-usual day
Other menopause symptoms: hot flashes, mood changes, fatigue, or brain fog
Treatments and relief tools: heat, medication, physical therapy exercises, or rest
These notes work like puzzle pieces. One note alone may not tell you much. Two or three weeks of notes often show patterns you would not remember accurately on your own.
A single tool also lowers friction. Instead of spreading clues across a notes app, calendar, and your memory, Lila's menopause symptom tracking plan gives you one place to log symptoms, routines, and progress while following a personalized plan.
Why digital support helps with follow-through
Joint pain plans often break down for ordinary reasons. You forget which exercise felt good. You cannot remember whether the flare started before or after a stretch of bad sleep. You skip routines for a few days, then assume nothing was working anyway.
Digital tracking helps by making the plan visible. Reminders support consistency. Trend views help you spot whether you are improving slowly, even if day-to-day symptoms still bounce around. Guided prompts can also make appointments more useful because you are bringing patterns, not guesses.
That is often the primary value. Less trial and error. More informed decisions about what to keep, what to adjust, and what to discuss with your clinician.
When to See a Doctor and Your Path Forward
Menopause-related joint pain is common, but that doesn't mean you should just live with it. A strong plan usually combines medical guidance, strength-building, low-impact movement, sleep support, and symptom tracking. That's the most practical way to approach joint pain in menopause treatment without relying on a single fix.
Do seek medical care sooner if any of these red flags show up:
Sudden severe pain: especially if you can't bear weight or move the joint normally
Visible redness, heat, or major swelling: these can suggest something beyond routine menopause-related discomfort
Fever with joint pain: this needs prompt evaluation
One-sided calf swelling or pain: don't assume it's just stiffness
Pain after a fall or injury: even if it seems minor at first
Numbness, weakness, or loss of function: especially if symptoms are progressing
Persistent pain that disrupts daily life or sleep: if it's not improving, it deserves a fuller workup
You don't need to choose between "it's nothing" and "something is seriously wrong." There's a middle ground where symptoms are real, treatable, and worth discussing. With the right support, many women can move better, sleep better, and feel more like themselves again.
If you're ready for more structure and less guesswork, Lila can help you track symptoms, spot patterns, and follow a personalized menopause plan that fits real life. It's a simple way to turn daily check-ins into useful insight, especially when joint pain, sleep, mood, and energy are all shifting at once.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.