Effective Perimenopause Diet for Weight Loss
Struggling with perimenopause weight gain? Discover an evidence-based, sustainable perimenopause diet for weight loss. Get your effective plan!
If you're eating “pretty well,” trying to exercise, and still watching your waistline change, you're not imagining it. Many women reach their 40s or 50s feeling like their body has stopped responding to the same habits that worked for years. The usual advice to just eat less and move more often feels incomplete, because during perimenopause, it is.
A good perimenopause diet for weight loss has to do more than cut calories. It has to protect muscle, steady energy, support symptom management, and adapt to the way your body is changing from month to month, or even week to week. Generic meal plans miss that reality.
The most useful plan is one you can adjust using your own data: hunger, sleep, bloating, cravings, cycle shifts, hot flashes, and energy patterns. That’s how weight loss becomes more sustainable. It stops being a punishment and starts becoming informed decision-making.
Why Perimenopause Changes Your Body Composition
The frustration is real. Women in perimenopause often tell me, “I haven’t changed that much, but my body has.” That mismatch between effort and outcome is one of the clearest signs that physiology has changed.
Women in perimenopause experience an average weight gain of 1.5 pounds (approximately 0.68 kg) per year between ages 45 and 65, driven by estrogen decline, muscle loss of 3 to 4%, increased insulin resistance, and a shift toward central fat storage, as summarized in this review on perimenopausal and postmenopausal weight loss challenges.
Estrogen changes where weight shows up
One of the most noticeable changes is fat redistribution. Even without dramatic changes in food intake, many women start storing more fat around the abdomen instead of the hips or thighs. That’s not a lack of willpower. It’s a hormonal shift.
Estrogen doesn’t just affect periods and hot flashes. It also influences insulin sensitivity, appetite patterns, and where the body prefers to store energy. When estrogen becomes less predictable, body composition often changes before the scale changes much.
Your body may be following different biological rules now. That means your strategy needs to change too.
For some women, this shows up as a thicker waist despite stable weight. For others, it looks like slow, steady gain that seems disconnected from what they’re eating. Both experiences are common.
Muscle loss quietly lowers your metabolic buffer
The second issue is sarcopenia, or age and hormone-related muscle loss. Muscle is metabolically active tissue. When you lose it, your body has less of a buffer against weight gain.
Many women respond by eating less and doing more cardio. That can backfire. If the plan strips away more lean mass, it makes future weight loss harder and often increases fatigue, cravings, and frustration.
That’s why any serious perimenopause diet for weight loss has to start with one question: how do we preserve muscle while reducing fat mass? If the answer is missing, the plan is incomplete.
For a broader conversation on this changing physiology, this interview with a women's health expert on menopause and weight loss is a useful companion read.
Insulin resistance changes the feel of hunger and energy
The third shift is insulin resistance, leading many women to notice that they tolerate sugary snacks, refined carbs, or long gaps without food differently than they used to. A breakfast that once felt fine may now lead to a late-morning crash. An afternoon snack habit may turn into evening overeating.
You don’t need to fear carbohydrates. But you do need to use them more intentionally. During perimenopause, food quality and meal structure often matter more than they did before.
A few signs that body composition is changing in a hormone-driven way:
Waist gain first: pants feel tighter at the midsection before the scale moves much.
Less recovery: hard workouts leave you more depleted instead of energized.
More hunger swings: meals without enough protein or fiber stop holding you.
Same habits, different outcome: your old routine no longer maintains your weight.
Why “eat less” often fails
If your body is losing muscle, storing more centrally, and handling blood sugar less efficiently, aggressive restriction usually makes things worse. It may produce short-term loss, but often at the expense of muscle, mood, sleep, and adherence.
That’s why women often feel stuck in perimenopause. They’re using a strategy built for a different hormonal environment.
The answer isn’t to chase perfection. It’s to build a plan that reflects what your body needs now: enough protein, enough fiber, enough nutrients, a modest calorie deficit, and enough flexibility to adjust when symptoms shift.
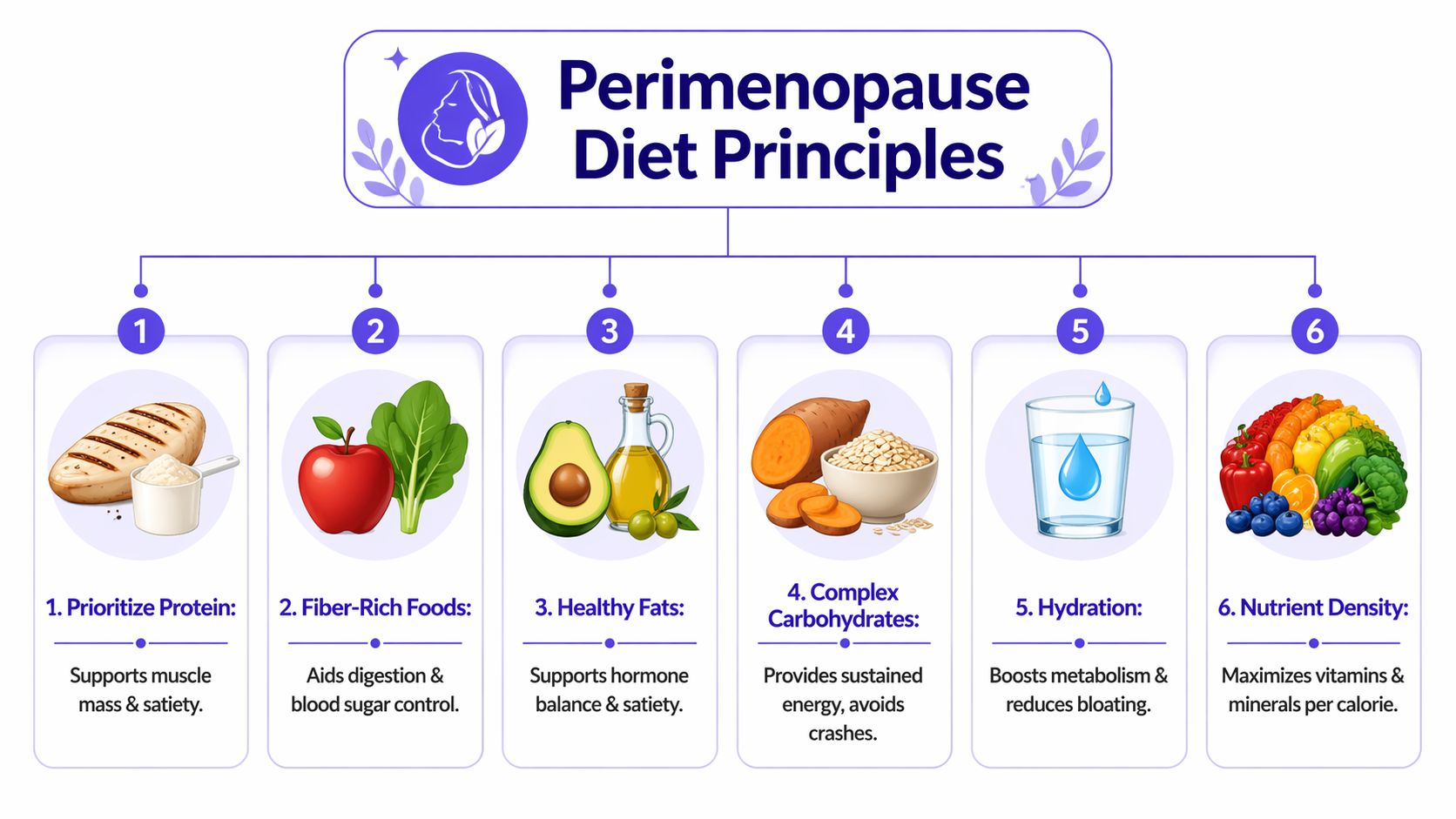
The Core Principles of Your Perimenopause Diet
A workable plan needs structure, but it shouldn’t feel rigid. I like to use a simple visual I call the Perimenopause Plate. It keeps meals balanced without forcing obsessive tracking.
Think of most meals like this:
Half the plate: non-starchy vegetables
One quarter: protein-rich foods
One quarter: high-fiber carbohydrates
That framework is simple enough for busy days and sturdy enough to support weight loss.
A balanced hypocaloric diet that creates a 500 kcal daily deficit, enriched with iron, calcium, and phytoestrogens from 5 daily servings of fruits and vegetables plus high-fiber foods like nuts, whole cereals, and pulses, is described as a recommended nonpharmacological approach for perimenopausal women in this overview of weight loss programs for women and tailored approaches.
Protein comes first
Protein is the anchor. During perimenopause, intake should rise to 1.2 to 1.6 g/kg body weight daily across meals to help counter muscle loss and improve satiety, as noted in the evidence summarized in the earlier section’s clinical review.
In practice, that means you stop treating protein like a dinner-only nutrient. Breakfast and lunch matter just as much. If the first half of your day is mostly toast, fruit, coffee, and snacks, hunger often rebounds later.
Useful protein options include:
Animal proteins: eggs, Greek yogurt, cottage cheese, chicken, turkey, fish
Plant proteins: tofu, tempeh, edamame, lentils, beans
Convenience proteins: pre-cooked chicken, tinned fish, plain skyr, roasted edamame
Practical rule: Build the protein part of the meal first, then add vegetables, smart carbs, and fats around it.
Fiber and carbohydrate quality shape appetite
Many women don’t need fewer carbs. They need better-structured carbs. High-fiber sources tend to support steadier energy and better appetite control than refined choices eaten on their own.
That’s why the carbohydrate quarter of the plate works best when it includes foods like oats, beans, lentils, quinoa, brown rice, or starchy vegetables. These are easier to build around than a grazing pattern of crackers, granola bars, or pastries.
If you want ideas for which foods tend to work well in this stage, Lila’s guide to best foods for perimenopause is a practical reference.
Healthy fats matter, but they’re not a free-for-all
Fat supports satisfaction and meal quality, and it helps food feel normal instead of clinical. But portions can often become larger than intended.
Use fats intentionally:
For cooking: olive oil, avocado oil
For meals: nuts, seeds, avocado, tahini, olives
For weekly rotation: oily fish when you enjoy it
A small amount can make a meal satisfying. A “healthy” meal loaded with nuts, nut butter, oil, cheese, and avocado can still push your energy intake beyond what supports fat loss. That’s not a moral issue. It’s just portion math.
Some women also like including green tea as a low-sugar drink option. If you're exploring that route, this overview of the best green tea for weight loss can help you compare choices without turning it into a miracle fix.
Don’t chase the lowest calorie target
A modest deficit works better than a severe one for most women in this stage. The goal is to reduce fat mass while keeping your energy, training capacity, and adherence intact.
What usually works better than strict dieting:
Regular meals instead of long chaotic gaps followed by overeating.
Small frequent portions when large meals worsen bloating or energy dips.
Nutrient density over “diet foods.”
Processed foods in context, not total elimination.
The diets that fail most often in perimenopause are the ones that ask too much of an already stressed body. If a plan leaves you cold, exhausted, obsessed with food, and less able to exercise, it’s not a good plan just because it’s disciplined.
Building Your Personalized Meal Plan
A good meal plan shouldn’t feel like homework. It should feel like a template you can repeat, swap, and adjust when life gets messy. The easiest way to build one is to stop asking, “What’s the perfect diet?” and start asking, “What meals keep me full, steady, and consistent?”
Below is a simple example of how a perimenopause diet for weight loss can look over three days. It isn’t a prescription. It’s a model.
Sample 3-Day Perimenopause-Friendly Meal Plan
Meal | Day 1 | Day 2 | Day 3 |
|---|---|---|---|
Breakfast | Greek yogurt with berries, chia seeds, and oats | Veggie omelet with toast and fruit | Protein smoothie with spinach, frozen berries, plain yogurt, and flax |
Lunch | Salmon bowl with greens, quinoa, cucumber, and olive oil dressing | Lentil soup with side salad and seeded crackers | Chicken salad wrap with crunchy vegetables and hummus |
Dinner | Chicken, roasted vegetables, and brown rice | Tofu stir-fry with mixed vegetables and edamame | Baked fish, sweet potato, and sautéed greens |
Snack | Apple with nuts | Cottage cheese with fruit | Roasted chickpeas or yogurt with seeds |
A realistic day of eating
The pattern matters more than the exact food. Breakfast includes protein, not just carbohydrates. Lunch is built to prevent the late-afternoon crash. Dinner is balanced enough that you don’t keep circling the kitchen afterward.
Many women often get stuck in this pattern: they eat lightly all day because they’re “being good,” then hunger catches up at night. The fix usually isn’t more discipline. It’s a better breakfast and lunch.
Here are a few useful swaps that preserve the structure without making meals repetitive:
Instead of oats, try quinoa porridge or seeded toast with eggs.
Instead of chicken, use tofu, beans, lentils, or tinned fish.
Instead of rice, rotate potatoes, barley, or whole-grain pasta.
Instead of a sweet snack, pair fruit with yogurt, cheese, or nuts for more staying power.
If a meal leaves you hungry within a short time, it usually needs more protein, more fiber, or both.
Quick-prep options for busy weeks
You do not need elaborate recipes for this to work. Most women do better with repeatable building blocks than with ambitious meal plans that collapse by Thursday.
A simple prep strategy:
Cook one protein ahead: chicken, tofu, lentils, turkey meatballs, boiled eggs
Wash and cut vegetables: so lunch takes minutes, not motivation
Keep one easy carb ready: cooked rice, potatoes, grain mix, or wraps
Stock fallback meals: soup, frozen vegetables, tinned beans, yogurt, eggs
If snacking is where things unravel, it helps to keep better defaults on hand. This roundup of healthy snacks for weight loss offers ideas that are easier to build into a practical routine than relying on whatever is nearby.
Personalization matters more than meal perfection
Two women can eat equally “healthy” diets and get very different results if one skips protein at breakfast, sleeps poorly, and crashes every afternoon while the other eats in a more stable rhythm. That’s why personalization matters.
Use these questions to shape your version of the plan:
Question | What to notice | Possible adjustment |
|---|---|---|
Are you hungry soon after breakfast? | Low satiety in the morning | Add more protein or fiber |
Do you crash mid-afternoon? | Lunch may be too light or too refined | Add protein, vegetables, and a steadier carb |
Do evenings feel snacky? | Earlier meals may be under-fueling | Increase lunch or dinner satisfaction |
Do large meals worsen bloating? | Meal size may be the issue | Try smaller, more frequent meals |
If you still have cycles, you may also notice that appetite, cravings, or digestion change at different times of the month. That’s useful information, not inconsistency. It means your plan should flex.
The women who do well long term usually aren’t the ones with the strictest meal plan. They’re the ones who can adapt without abandoning the structure.
Fine-Tuning Your Plan with Symptom Tracking
Most weight loss advice ignores the most useful source of information you have: your own pattern data. During perimenopause, symptoms often shift faster than your plan does. That’s why tracking matters.
Precision nutrition apps are using data to customize 10 to 12 hour eating windows, helping the 60 to 70% of perimenopausal women with disrupted sleep cycles avoid dawn cortisol peaks, while allowing adjustments based on symptom monitoring via apps, according to this discussion of the best diet for perimenopause.
Tracking doesn’t need to mean obsessive logging. It means noticing cause and effect. Food, symptoms, sleep, energy, and cycle changes all influence one another. If you don’t capture them, the pattern stays hidden.
What to track each day
A useful daily check-in is short. You’re looking for trends, not creating a second job.
Track things like:
Meals and snacks: rough timing and what you ate
Energy: morning, afternoon, evening
Symptoms: bloating, hot flashes, headaches, cravings, mood shifts
Sleep: how rested you felt
Cycle changes: if you’re still bleeding, spotting, or noticing timing shifts
If you want a dedicated tool for this, a menopause symptom tracker app can help centralize those patterns instead of leaving you to piece them together across notes, calendars, and memory.
How to read your own patterns
Once you have a few weeks of notes, useful questions emerge.
If you’re bloated, look back at the previous couple of days. Did fiber jump suddenly? Did you eat more takeaway foods? Did you go long stretches without water or regular meals?
If your energy drops hard in the afternoon, examine lunch. Was it mostly carbohydrates? Was protein missing? Did you eat too little because you were busy?
If hot flashes feel worse on certain days, check the broader context. Poor sleep, higher stress, irregular eating, and alcohol often travel together.
The point of tracking isn’t to prove you’re doing something wrong. It’s to identify what your body responds to.
Here’s a simple way to use symptom data in real time:
Spot one repeating issue. Afternoon crash, night cravings, bloating, sleep disruption.
Review the lead-up. What happened with food, stress, sleep, and movement?
Change one variable. Add protein at breakfast, shift lunch composition, shorten the eating window gently, or move dinner earlier.
Watch the response. Give the change enough time to reveal a pattern.
A short visual walkthrough can help make this process easier to picture:
▶ PlayAdapting the plan around your cycle and symptoms
Perimenopause is variable by definition. That means your eating pattern may need to be variable too.
Examples of sensible adjustments:
Heavier period week: emphasize iron-rich meals and don’t under-eat if appetite rises.
Poor sleep stretch: use a gentler eating window and prioritize steadier meals over aggressive fasting.
Bloating phase: reduce meal volume, choose simpler meals, and spread fiber more evenly.
Low-energy week: lean on convenience meals instead of skipping meals and then overeating later.
This is the part most generic plans miss. Your body isn’t static, so your plan can’t be static either. One woman may do well with a structured eating window. Another may find that rigid fasting worsens stress and rebounds into overeating. The right answer is the one your data supports.
Beyond the Diet Lifestyle Strategies for Success
Food matters, but diet alone rarely solves perimenopause weight gain. If you ignore movement, stress, and sleep, you’re working against your own biology.
There’s also a strong symptom payoff to modest progress. Losing 5 kg (11 pounds) in overweight perimenopausal women improves hot flash tolerability by 30%, and in the Women’s Health Initiative study of 17,473 women ages 50 to 79, a low-fat diet pattern made women 3 times more likely to lose at least 5 pounds and twice as likely to eliminate hot flashes after one year, as reported in this PMC review of weight management and vasomotor symptoms.
Strength training protects what dieting often sacrifices
When women focus only on eating less, they often lose weight without improving body composition the way they hoped. Strength training changes that. It helps preserve or rebuild lean mass, supports insulin sensitivity, and often improves how the body looks and functions even before major scale changes happen.
The target doesn’t need to be extreme. A consistent routine built around resistance is more useful than occasional hard workouts followed by long gaps. If you need a place to start, Lila’s guide to best exercises for menopause covers practical options.
Stress changes appetite and consistency
High stress doesn’t just affect mood. It alters appetite, food choices, patience, sleep, and recovery. Women often blame themselves for “falling off track” when the actual issue is that their nervous system is overloaded.
That’s why your plan should include stress reduction that is realistic enough to keep using:
Walking: especially after meals or during high-stress days
Short breathing resets: before meals if you tend to eat fast
Lower-friction exercise weeks: when sleep is poor
Boundaries around overdoing it: hard training isn’t always the right answer
More effort isn’t always better. Better recovery often produces better adherence.
Sleep is a metabolic tool
Poor sleep makes hunger louder, patience shorter, and cravings harder to manage. It also makes training feel harder and planning feel optional. In perimenopause, that creates a cycle quickly.
A few practical changes often help:
Keep dinner satisfying, not skimpy
Avoid letting caffeine drift too late
Create a repeatable wind-down routine
Use symptom tracking to notice what worsens sleep
Women usually make the best progress when these three pillars support each other. Eat in a way that steadies energy. Move in a way that protects muscle. Recover in a way that lowers stress and improves sleep.
Common Pitfalls and How to Stay on Track
The biggest mistake I see is all-or-nothing thinking. One high-calorie meal becomes “I’ve blown it,” and that turns into a weekend of giving up. Perimenopause doesn’t respond well to that cycle.
Another problem is trying to outrun biology with increasingly restrictive plans. Repeated dieting can slow basal metabolic rate by 5 to 10% in perimenopause, and recovery protocols described in this discussion of perimenopause nutrition note that women with a dieting history may need 1.6g/kg protein plus resistance training to rebuild lean mass and stabilize weight without extreme calorie cuts.
What commonly backfires
Skipping meals to “save calories” often leads to evening overeating.
Cutting calories too hard can reduce energy, training quality, and adherence.
Relying only on the scale hides progress in body composition, energy, and symptom relief.
Changing everything at once makes it hard to know what’s helping.
A steadier mindset works better
If you’ve dieted for years, your first job may not be to push harder. It may be to rebuild trust with food structure and recover consistency.
Use better markers of progress:
Clothes fit
Energy stability
Fewer cravings
Better workouts
Improved sleep
Less symptom volatility
Quick fixes usually ask you to sacrifice the very things that help weight loss last, namely muscle, energy, and consistency.
When a day goes off plan, return to the next meal. Not Monday. Not next month. The next meal. That skill matters more than perfect compliance ever will.
Frequently Asked Questions
Can I still drink alcohol and lose weight?
Yes, but it can make the process harder if it disrupts sleep, increases appetite, or leads to less structured eating. The most useful approach is to notice your own response rather than turning it into a moral issue.
What supplements are most effective for perimenopause weight loss?
No supplement replaces the basics of protein, meal structure, fiber, movement, sleep, and stress management. Supplements may have a role in overall care, but weight loss during perimenopause is usually driven more by habits than by pills or powders. Discuss supplements with your clinician, especially if symptoms or fatigue are significant.
How long will it take to see results?
That depends on your starting point, symptom load, sleep, stress, and whether your plan is realistic enough to sustain. In practice, early wins often show up first as steadier energy, fewer cravings, better digestion, or improved sleep before major visible changes.
When should I talk to my doctor about weight gain?
Talk to your doctor if weight gain feels sudden, symptoms are severe, your periods change dramatically, fatigue is significant, or your usual efforts aren’t matching your health picture. Medical review matters if something beyond perimenopause may be contributing.
If you want a more adaptive approach than a generic meal plan, Lila can help you track symptoms, meals, sleep, energy, and cycle changes in one place so you can adjust your perimenopause diet for weight loss based on your actual patterns, not guesses.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.