Vitamin D and Menopause: A 2026 Health Guide
Explore the link between vitamin d and menopause. Learn how it impacts bones, mood, and weight, plus get expert guidance on testing, dosing, and tracking.
You wake up tired even after a full night in bed. Your patience feels thinner. Your joints ache in a way they didn’t a year ago. Maybe your periods are changing, or maybe they’ve become unpredictable enough that you keep wondering, “Is this perimenopause, stress, or something else?”
That confusion is common in your 40s and 50s. Menopause doesn’t arrive with one neat symptom. It often shows up as a cluster of subtle shifts in energy, mood, sleep, body temperature, and body composition. One of the most overlooked pieces in that puzzle is vitamin D.
Vitamin D is widely known as the “bone vitamin.” That’s only part of the story. During the menopause transition, vitamin D affects far more than your skeleton. It interacts with hormones, calcium absorption, vaginal tissue, and possibly the timing of menopause itself. One analysis of NHANES data found that vitamin D deficiency increased the likelihood of early menopause by 34% (analysis summary).
That doesn’t mean vitamin D explains every symptom. It doesn’t. It also doesn’t mean a supplement is a cure-all. The useful question is more specific: what can vitamin d and menopause care realistically do together, and where should you keep your expectations modest?
A practical, evidence-based approach helps. Instead of hoping vitamin D will fix everything, you can use it for the areas where it has the strongest support, pay attention to symptoms it likely won’t change much, and track your own pattern over time.
Navigating Menopause with the Sunshine Vitamin
Many women first pay attention to vitamin D after a bone scan, a fracture, or a lab result comes back low. By then, the conversation can feel too narrow.
During perimenopause and after menopause, vitamin D deserves a wider look. It supports systems that often start feeling less steady during this transition, especially bone health and, for some women, mood. At the same time, it is not a cure-all. If you are hoping it will solve every symptom, especially hot flashes, the evidence does not support that.
A more practical way to look at vitamin d and menopause is this: vitamin D may be one piece of the puzzle, not the whole puzzle. Hormones are shifting. Sleep may be worse. Stress may be higher. Nutrient gaps can sit on top of all of that, like static layered over an already fuzzy radio signal.
Earlier in the article, we noted research linking vitamin D deficiency with a higher likelihood of early menopause. Deficiency is also common in postmenopausal women. That detail is significant for a woman already noticing cycle changes, new fatigue, or a mood shift that feels hard to explain.
Menopause symptoms and nutrient deficiencies can overlap. When low mood, body aches, fatigue, and changing cycles show up together, it makes sense to check both hormones and vitamin status.
Why this gets missed
Vitamin D deficiency rarely announces itself clearly. It often shows up in ways that are easy to misread or dismiss:
General fatigue that sounds like stress or poor sleep
Muscle aches or weakness that get blamed on aging or exercise
Mood changes that seem tied only to life pressure
Bone loss that stays silent until much later
That overlap creates a real diagnostic gray zone. A woman can be in perimenopause and low in vitamin D at the same time, and the symptom picture can blur.
This is one reason broad advice can fall short. “Take vitamin D for menopause” is too vague to be useful. A better question is whether low vitamin D could be making specific problems worse, and whether those problems are the ones vitamin D is known to affect.
A more useful mindset
Start with three questions:
Could low vitamin D be making this transition harder on my bones, muscles, or mood?
Which symptoms are realistic to expect improvement in, and which probably need a different strategy?
What should I track, such as symptoms, supplements, and lab results, so I can judge whether a change is helping?
That approach turns vitamin D from a vague wellness idea into something you can apply. It also sets up a more personalized plan, especially if you track patterns over time in a tool like Lila instead of relying on memory alone.
The Hormone That Acts Like a Vitamin
Vitamin D is called a vitamin, but in the body it behaves more like a hormone-like signaling molecule. A helpful analogy is an orchestra conductor. Calcium, bone cells, gut cells, immune cells, and reproductive tissues may all be the musicians. Vitamin D helps coordinate when and how some of them perform.
That matters more in menopause because estrogen used to support several of the same systems. When estrogen declines, the body loses some of that backup.
Why bone health changes so fast after menopause
One of vitamin D’s most important jobs is helping the gut absorb calcium. Mechanistically, vitamin D enhances calcium absorption by 30% to 40%, and menopause makes this process less efficient because estrogen decline interferes with it. That’s part of why women can lose 2% to 3% of bone mass annually after menopause (mechanism overview).
Think of estrogen and vitamin D as two staff members working the same warehouse door. Estrogen helps keep the loading dock running smoothly. Vitamin D helps bring calcium inside. When estrogen drops, the door gets harder to manage. If vitamin D is also low, even less calcium gets where it needs to go.
Vitamin D and estrogen work in parallel
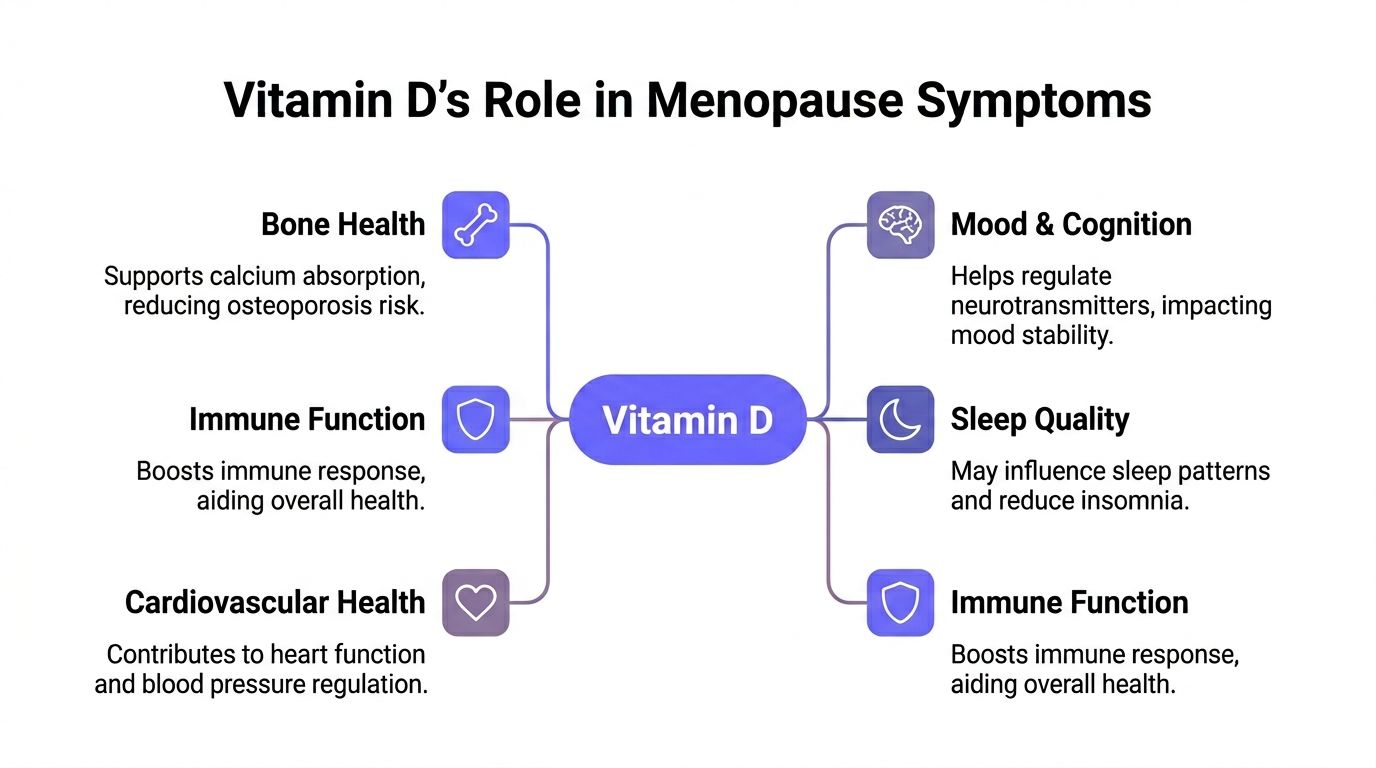
Vitamin D doesn’t replace estrogen. But it affects several areas that become more vulnerable as estrogen falls:
Calcium handling
Bone remodeling
Muscle function
Tissue maintenance in the genitourinary tract
Some brain and immune signaling pathways
That’s why low vitamin D can feel more noticeable in midlife than it did in your 20s.
Why “normal aging” isn’t the whole story
Many women are told to expect aches, lower energy, or more stiffness with age. Some change is normal. But “normal” doesn’t mean “nothing to evaluate.”
If vitamin D is low, the body may struggle more with tasks that already become harder during menopause. It’s not magic. It’s basic physiology. You need enough vitamin D on board for calcium to be absorbed efficiently and for certain tissues to function the way they’re meant to.
Practical rule: When estrogen declines, vitamin D matters more, not less.
The takeaway for everyday life
This helps explain why one woman notices bone or muscle issues early, while another mainly notices mood shifts or vaginal dryness. Menopause is not a single-track experience, and vitamin D isn’t a single-purpose nutrient.
The key is to stop thinking of it as just a bone supplement. In midlife, it’s part of a larger hormonal and metabolic conversation.
How Vitamin D Impacts Key Menopause Symptoms
A common midlife pattern looks like this: your hot flashes get the blame for everything, but the full picture is messier. You may also have low bone density, a flatter mood, more body aches, or poor sleep that started around the same time. Vitamin D can be part of that picture, but it does not explain every symptom.
The most useful way to look at vitamin D in menopause is to sort symptoms into three buckets:
Symptoms it clearly supports: bone health, and sometimes muscle function
Symptoms it may influence indirectly: mood, energy, and sleep in women who are low
Symptoms it usually does not fix on its own: hot flashes and night sweats
That framework matters because it keeps expectations realistic.
Where vitamin D has the strongest case
Bone is the clearest example. Bone works like a savings account. Before menopause, estrogen helps protect your balance. After menopause, withdrawals happen faster. If vitamin D is low, your body has a harder time absorbing and using calcium well, which makes that loss harder to slow.
You usually cannot feel bone loss day to day. That is why vitamin D can be important even when the symptom is silent.
Muscle function also deserves a brief mention here. Some women with low vitamin D notice more weakness, less steadiness, or a heavier, achier feeling in the body. That does not prove vitamin D is the only cause, but it can be one piece of why stairs, workouts, or long walks feel harder than they used to.
Where vitamin D may help, but only in context
Mood and sleep are the areas that create the most confusion online.
Low vitamin D is often found alongside low mood, fatigue, and poor sleep. But association is not the same as cause. A supplement is more likely to help if you are deficient than if your level is already adequate. In other words, vitamin D is more like fixing a missing battery than pressing a magic reset button.
Sleep follows the same logic. If low vitamin D is contributing to body aches, low mood, or general malaise, correcting it may help sleep improve over time. If you are waking from classic vasomotor symptoms, that is a different mechanism. Women searching for natural ways to relieve hot flashes usually need a more targeted plan.
Night sweats can blur this distinction because they disrupt sleep so dramatically. If that is your main problem, start by asking the more specific question, why do I sweat in my sleep, instead of assuming vitamin D is the answer.
What this means in real life
Vitamin D is best used as a support tool, not a catch-all menopause treatment.
A practical way to judge whether it belongs on your priority list is to look for patterns such as:
Bone loss, osteopenia, or fracture risk
Muscle aches or weakness
Low mood or fatigue along with other signs of deficiency
Sleep that feels worse because of pain, discomfort, or low energy rather than heat surges alone
This is also where tracking helps. If you log symptoms, vitamin D intake, and lab results in an app like Lila, you can stop guessing. You may notice that improving a low vitamin D level lines up with better energy or fewer aches, while hot flashes stay exactly the same. That kind of pattern is useful. It shows you what vitamin D can realistically do for your body, and where you need a different strategy.
Symptom area | What vitamin D can realistically do |
|---|---|
Bones | Strong support, especially if levels are low |
Muscles | May improve strength, aches, or steadiness in some women with deficiency |
Mood and energy | May help if deficiency is part of the problem |
Sleep | May help indirectly when pain, low mood, or discomfort are involved |
Hot flashes and night sweats | Usually not a reliable stand-alone treatment |
The goal is accuracy. Vitamin D matters in menopause, but it helps most when you match it to the right symptom.
The Surprising Truth About Vitamin D for Hot Flashes
Hot flashes get a lot of attention because they’re disruptive, visible, and exhausting. When they hit at work, wake you from sleep, or leave you drenched at night, it’s natural to look for a nutrient solution. Vitamin D often gets pulled into that search.
The problem is that the evidence doesn’t strongly support vitamin D as a reliable treatment for vasomotor symptoms like hot flashes and night sweats.
Large trials from the Women’s Health Initiative, involving over 34,000 women, found that standard vitamin D and calcium supplementation did not improve hot flashes, mood, or sleep quality compared with placebo in postmenopausal women (WHI summary).
That can feel disappointing, but it is useful. It helps you stop spending energy on weak strategies and focus on interventions more likely to help.
Why this matters
If your main complaint is sudden heat, flushing, and night sweats, vitamin D probably shouldn’t be your first-line fix. It may still matter for your overall health, but it’s not the same as a targeted hot flash treatment.
Women often get confused here because low vitamin D can overlap with fatigue, low mood, and body discomfort. If those improve, someone may feel better overall and assume vitamin D treated the hot flashes themselves. Sometimes it improved the background stress on the body, not the vasomotor symptom directly.
A better way to think about night sweats
Night sweats can have more than one trigger. Menopause is common, but it’s not the only explanation. If you want a broader primer on other possible causes, this guide on why do I sweat in my sleep is a useful starting point.
If your symptoms clearly fit the menopause pattern, it makes sense to look at dedicated strategies for vasomotor relief. Lila’s article on natural hot flash relief gives a practical overview of non-drug options women often explore.
If hot flashes are your main target, choose treatments aimed at hot flashes. Keep vitamin D in the plan for bone and whole-body health, not as your primary rescue tool.
The trust-building truth
Good menopause care isn’t about making one nutrient sound powerful enough to do everything. It’s about matching the right tool to the right symptom.
Vitamin D deserves a place in that plan. It just doesn’t deserve all the credit.
Are You Deficient? Testing and Safe Supplementation
By the time many women test vitamin D, they’ve already spent months feeling run down. They may describe themselves as tired, achy, flat, or fragile, but not “sick” enough to seek a workup right away. That’s why testing matters. It replaces guessing with something measurable.
The lab test to ask about is 25-hydroxyvitamin D, often written as 25(OH)D. That’s the standard blood marker used to assess vitamin D status.
What symptoms might point to low vitamin D
Vitamin D deficiency can be easy to miss because the signs are broad. In midlife, it can overlap with menopause so closely that women may assume it’s all hormonal.
Clues worth discussing with a clinician include:
Bone or muscle aches
Persistent fatigue
Low energy for exercise
A history of low bone density, osteopenia, or fracture
Vaginal dryness or irritation that seems to worsen with menopause
Limited sun exposure or dietary intake
One area that deserves more attention is genitourinary syndrome of menopause, often called GSM. Research summarized in a review found that for GSM, vitamin D can improve vaginal atrophy symptoms, and high-dose oral or vaginal use has been associated with reduced dryness and fewer UTIs in some settings (GSM review).
A simple table for lab conversations
Below is a practical framework you can use when talking with your clinician. The exact interpretation may vary by provider, especially if you have osteoporosis, kidney disease, malabsorption, or other medical factors.
Status | Blood Level (ng/mL) | Blood Level (nmol/L) | General Daily Intake (IU) |
|---|---|---|---|
Deficient | Below 20 | Below 50 | Discuss a clinician-guided plan |
Insufficient | 20 to 29 | 50 to 74 | Intake may need review with your clinician |
Sufficient | 30 and above | 75 and above | Maintenance needs vary |
Higher target used in some menopause discussions | 40 to 60 | 100 to 150 | Only use a targeted plan with clinician guidance |
That higher target appears in some menopause-oriented discussions, but it isn’t a reason to self-prescribe aggressively. More isn’t always better.
D2, D3, and dosing questions
If you do supplement, many clinicians prefer vitamin D3 over D2. You may also see dosing written in IU, which stands for international units.
The safest path is usually straightforward:
Get tested
Review the result in the context of your symptoms
Match the dose to the deficiency level and your health history
Recheck when your clinician recommends
If your clinician orders a broader panel to look at fatigue, electrolytes, liver markers, or metabolic health, it can help to understand how those labs fit together. Carter's guide to CMP testing gives a readable overview of one common blood test panel women may see alongside other evaluations.
A note on menopause testing
If you’re not sure whether symptoms are from perimenopause, menopause, or something else, a symptom-focused conversation often matters more than a single hormone number. Lila’s article on how to test for menopause is a useful overview of what lab work can and can’t tell you.
Clinical common sense: Don’t start with a megadose because social media said low vitamin D explains everything.
Safety first
Supplementation can be helpful. It still needs guardrails. Talk with your clinician before supplementing if you have kidney issues, sarcoidosis, a history of high calcium, or take medications that could affect vitamin D metabolism.
For vaginal symptoms, especially burning, repeated UTIs, pain with sex, or severe dryness, don’t assume a supplement alone is enough. GSM often responds best to a broader care plan that may include moisturizers, prescription treatment, pelvic care, or local estrogen, depending on your situation.
Getting Vitamin D From Sun Food and Supplements
A good vitamin D plan usually uses more than one source. Think of it as a three-part system: sunlight, food, and supplements. Each one helps fill a different gap.
Sunlight
Sun exposure can help your body produce vitamin D, but it’s not equally reliable for everyone. Season, latitude, skin tone, time outdoors, clothing, and sunscreen use all affect how much your skin can make.
That’s why two women with similar diets can have very different vitamin D levels. One walks outside most mornings. Another drives to work before sunrise, works indoors all day, and lives in a cloudy climate. Their bloodwork may look very different.
A practical way to use sunlight is to think in terms of regular, sensible exposure, not trying to “stockpile” sun on one weekend.
Food
Food usually won’t correct a major deficiency by itself, but it still matters because it helps create a more stable baseline. Vitamin D-containing foods also often fit nicely into a menopause-supportive eating pattern.
Common options include:
Fatty fish such as salmon, sardines, trout, or mackerel
Fortified dairy or plant milks
Fortified cereals
Eggs
Mushrooms, especially if they’ve been exposed to UV light
It also helps to remember that vitamin D works alongside calcium-rich foods and overall protein intake. If you’re trying to support bones, supplements alone won’t do the whole job.
Supplements
Supplements make sense when sun and food aren’t enough, or when a blood test confirms low levels. Consistency matters more than buying the most expensive bottle on the shelf.
When choosing a supplement, look for:
Vitamin D3 rather than D2, unless your clinician recommends otherwise
Clear labeling in IU
Third-party testing when possible
A dose that matches your actual need, not a random high number
If you’re building a broader menopause routine, this guide to best menopause supplements can help you think about vitamin D in the context of a full support plan rather than as a stand-alone fix.
Here’s a quick visual explainer if you want a simple refresher on how vitamin D works in the body and where supplements fit:
▶ PlayPutting the pieces together
The most sustainable strategy usually looks like this:
Source | Best use |
|---|---|
Sunlight | Background support when practical and safe |
Food | Daily foundation and habit support |
Supplements | Reliable correction or maintenance when intake and sun aren’t enough |
That approach keeps you from relying on a single tool for a problem that usually has multiple causes.
Your Action Plan for Tracking Vitamin D and Symptoms
You start vitamin D in January because your level came back low. By March, you are asking a very fair question: is anything changing?
That question trips up a lot of women in menopause because vitamin D usually works in the background. It is more like adjusting the thermostat than flipping on a light. Changes can be real, but gradual enough that memory blurs them.
What to track
A simple log is enough if you use it regularly. The goal is not perfection. The goal is pattern recognition.
Keep an eye on four things:
Supplement use
Write down the form, dose, and whether you took it with a meal.Symptoms vitamin D might realistically affect
Focus on energy, general body aches, mood, sleep quality, and vaginal dryness or discomfort. Those are more useful to track than symptoms vitamin D is unlikely to change, such as hot flashes.Sun and food patterns
A rough note is enough. More time outdoors one week and very little the next can help explain changes.Lab results
Keep your 25(OH)D level and test date in one place so you can compare symptoms with actual numbers.
How to avoid false conclusions
The biggest trap is changing everything at once. If you begin vitamin D, start strength training, clean up your diet, and begin hormone therapy in the same week, you will have a hard time sorting cause from coincidence.
A clearer method is to choose one main target symptom and one new step at a time. Then watch for several weeks. That gives you a cleaner read on what your body is responding to.
Three questions help:
What symptom am I hoping to improve first?
What change am I making right now?
How long will I track before I judge the result?
That last question matters. Hot flashes can push women to expect fast results from any new supplement. Vitamin D is usually not the answer for vasomotor symptoms, so a log can save you from waiting on the wrong fix.
Match the symptom to the strategy
This is the part many menopause articles skip. A better vitamin D level does not mean every symptom should improve.
If your lab value rises and your hot flashes stay the same, that does not automatically mean vitamin D "failed." It may still be helping with bone support, muscle discomfort, or mood, while your hot flashes need a different plan. On the other hand, if your energy, achiness, or vaginal comfort improve as your level improves, that pattern is worth paying attention to.
A symptom-tracking tool can make that easier. Lila is one example. It lets users log symptoms, sleep, meals, energy, and cycles in one place, which can help connect lab results and daily habits with how they feel.
Your body gives feedback slowly. Tracking helps you hear it more clearly.
A practical monthly review
At the end of each month, do a short check-in. Five minutes is enough.
Ask yourself:
Was I consistent with vitamin D?
Did energy, aches, mood, sleep, or vaginal comfort change at all?
Am I expecting vitamin D to help a symptom it probably does not affect, like hot flashes?
Do I need repeat labs or a conversation with my clinician about a different treatment?
That kind of review keeps wishful thinking and discouragement from running the show. It also gives you something more reliable than memory.
Menopause can feel messy. Tracking turns it into a series of observations you can practically use.
If you want a simpler way to connect symptoms, meals, sleep, cycle changes, and daily habits in one place, Lila offers an app-based approach to menopause tracking that can help you see patterns and make more informed conversations with your healthcare provider.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.