Painful Breasts During Perimenopause: Causes & Relief
Experiencing painful breasts during perimenopause? Understand the causes, learn effective self-care strategies, and know when to see a doctor. Get clarity now.

You wake up, roll over, and your breast hurts when it presses against the mattress. By midday, your bra feels too tight, your chest feels heavy, and your mind goes straight to the question almost every woman asks first. Is this normal, or is this something serious?
Painful breasts during perimenopause can be unsettling because they often show up without the familiar rhythm you may have known in your 20s or 30s. One month it feels like fullness and soreness in both breasts. Another time it's a sharp, localized twinge that seems to come out of nowhere. That unpredictability is exactly what makes it so stressful.
Understanding Perimenopausal Breast Pain
A woman in her 40s will often tell me some version of the same story. She wasn't expecting breast pain. She expected hot flashes, maybe irregular periods, maybe sleep changes. But suddenly her breasts feel swollen, sore, or oddly bruised, and now she's worried.
That worry makes sense. Breasts are an emotionally loaded part of the body, and new pain gets attention fast. The reassuring part is that this symptom is very common in midlife.
Up to 70% of women experience breast pain, known as mastalgia, at some point in their lifetime, with the highest prevalence among those in their 30s and 40s. Despite its prevalence, only 30% of affected women discuss it with doctors, according to Bonafide's overview of menopause and breast pain.
Why it catches women off guard
Perimenopause doesn't behave like a clean hormonal decline. Symptoms can appear, disappear, and return in a different form. Breast tenderness is one of the clearest examples of that pattern.
You might notice:
Heaviness or swelling that makes your usual bra uncomfortable
Tenderness to touch during exercise, sleep, or intimacy
Aching in both breasts that feels diffuse rather than pinpoint
Random sharper sensations that don't follow a neat monthly schedule
Breast pain during this stage is often more disruptive than dangerous.
That doesn't mean you should ignore it. It means you should approach it calmly. Most painful breasts during perimenopause are related to hormonal and tissue changes, not something ominous. The useful question usually isn't “Why is this happening to me?” It's “What pattern is my body showing me, and what helps?”
What deserves attention
Breast pain can be common and still deserve care. If it's affecting your sleep, exercise, mood, or ability to concentrate, it matters. If it's new, one-sided, or paired with another breast change, it deserves evaluation.
For many women, relief starts once the symptom stops feeling mysterious.
The Hormonal Rollercoaster Causing Your Breast Pain
Perimenopause hormones behave less like a dimmer switch and more like an old radio dial being turned too fast. The signal comes in, fades out, crackles, then blasts back unexpectedly. Your breasts are one of the tissues that react strongly to that static.
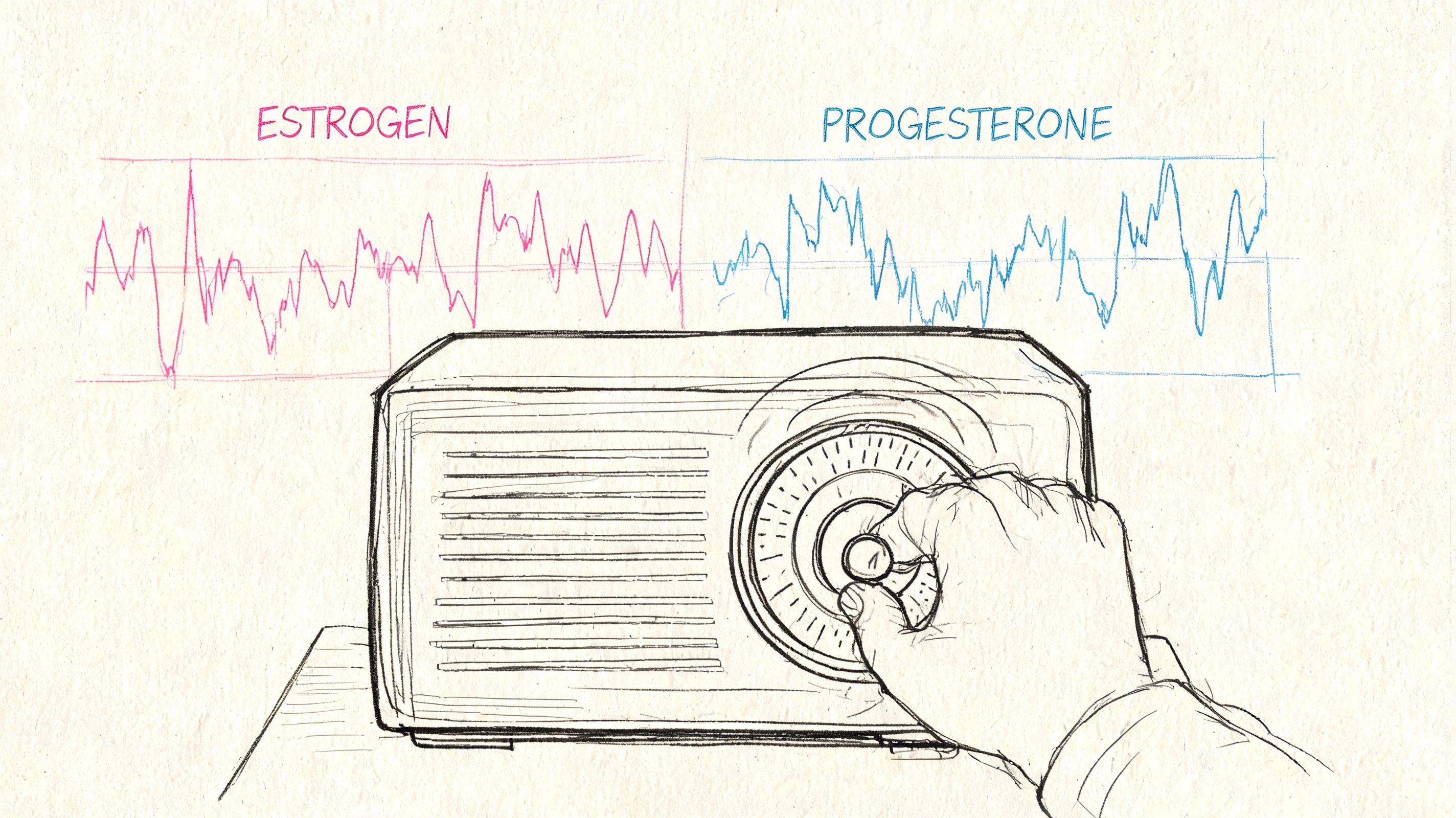
What estrogen is doing
The simplest explanation is this. During perimenopause, cyclical breast pain intensifies due to erratic fluctuations in estrogen and progesterone. Estrogen surges increase the size and number of ducts and milk glands, causing bilateral swelling and tenderness. This process is worsened in perimenopause due to unpredictable hormone spikes that can exceed levels seen during regular reproductive years, as described by Harvard Health on breast pain.
When estrogen surges, breast tissue can hold more fluid and feel fuller. Ducts and glandular structures become more reactive. That's why many women describe:
Fullness rather than just pain
Tenderness in both breasts
Swelling that changes from day to day
Pain that radiates toward the underarm
Progesterone complicates the picture. As ovulation becomes less consistent, progesterone often becomes less reliable too. That means estrogen's effects may feel less balanced, and breast tissue can become more sensitive.
Why it feels less predictable than PMS
Earlier in life, breast soreness may have shown up before a period and faded once bleeding started. During perimenopause, your hormones often stop following that tidy script.
That's why painful breasts during perimenopause can show up:
Before a period that arrives late
Without a clear period at all
In stronger waves than you used to feel
Alongside bloating, irritability, or poor sleep
If you've been trying to understand whether your symptoms line up with estrogen shifts, this guide to normal estradiol levels can help you put the bigger hormone picture into context.
A second factor often gets missed. Tissue support changes in midlife too. If your breasts feel heavier, exercise and daily movement can create more pull on ligaments and chest structures. That's one reason women often benefit from strength work and supportive movement habits. If that's part of your picture, these realistic post-menopausal fitness tips offer a grounded way to think about exercise without chasing extremes.
Here's a quick visual explanation of the hormone side of the story:
▶ PlayPractical rule: If soreness is moving, fluctuating, and tied to other perimenopause symptoms, hormones are high on the list of likely causes.
How Perimenopausal Breast Pain Is Different
Not all breast pain means the same thing. The symptom itself is common, but the pattern matters. That pattern often tells you whether you're dealing with typical hormonal tenderness, familiar PMS-type soreness, or a reason to get checked promptly.
What women usually notice
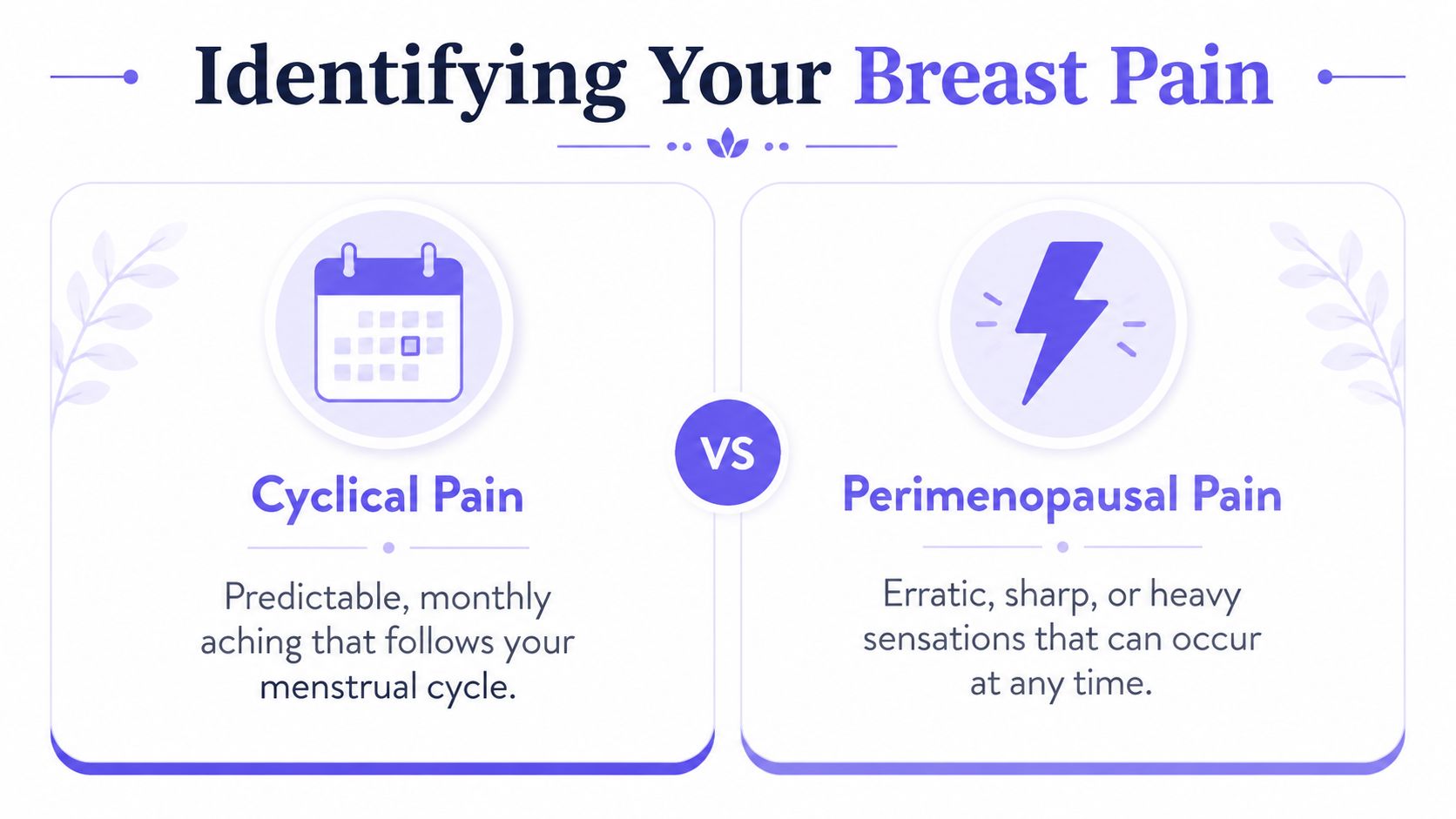
Perimenopausal breast pain can feel dull, burning, throbbing, heavy, swollen, or sharply tender. Some women notice it in both breasts. Others get one more sensitive area that comes and goes. The defining feature is often inconsistency.
Perimenopause's hormonal volatility leads to random soreness episodes, unlike predictable menstrual patterns. While mastalgia is a frequent concern, it's rarely linked to breast cancer, affecting fewer than 1 to 2% of cases. At the same time, 8 out of 10 breast cancers occur after age 50, which is why changing breast symptoms should be taken seriously without assuming the worst, as summarized by WebMD's review of breast changes in menopause.
Breast Pain Decoder
Symptom | Typical Perimenopause Pain | Typical PMS Pain | Potential Red Flag (See a Doctor) |
|---|---|---|---|
Timing | Irregular, can come and go unpredictably | Usually follows a familiar monthly pattern | Persistent and not changing |
Location | Often both breasts, sometimes diffuse | Often both breasts | One specific spot that stays painful |
Sensation | Heavy, swollen, burning, sharp, throbbing, tender | Achy, full, premenstrual soreness | Localized pain with another breast change |
Relation to cycle | Often unclear because cycles are shifting | Usually easier to predict | No obvious pattern and worsening |
What else is present | May come with sleep changes, mood changes, bloating, irregular bleeding | Often comes with usual PMS symptoms | Lump, nipple discharge, dimpling, visible skin change |
The key distinction
Typical PMS pain is familiar. Perimenopausal pain often feels less organized. That's what throws women off. It may be more intense, less timely, and harder to connect to a calendar.
A red flag pattern looks different. It tends to be persistent, focal, and paired with a physical change rather than generalized soreness.
If the pain moves around, fluctuates, or eases with cycle changes, it usually behaves differently from a concerning breast symptom.
That doesn't replace an exam. It gives you a better framework for what you're noticing in your own body.
Practical Self-Care for Easing Breast Tenderness
When breasts are painful, most women want relief first and theory second. That's reasonable. Self-care works best when it matches the source of the discomfort, whether that's swelling, ligament strain, friction, or a flare that's making already sensitive tissue feel overloaded.
Start with support
The most underestimated fix is often your bra.
If your breasts feel heavier or more swollen than usual, an underwire that normally feels fine can become irritating fast. A well-fitted, supportive, non-wired bra often helps because it reduces bounce, pressure, and ligament strain. This matters more during exercise, walking, stairs, and sleep.
Try these adjustments:
Switch the bra style to a soft but structured support bra on flare days
Use a sleep bra or soft crop top if turning in bed worsens pain
Recheck fit if your band or cup size seems suddenly wrong during symptom weeks
Use short-term comfort measures
These don't fix the cause, but they often lower the symptom burden enough to get through the day.
Cool compresses can calm swelling and tenderness
Warmth can help if muscle tension around the chest wall is part of the pain
Gentle movement may feel better than high-impact workouts during a flare
Topical anti-inflammatory options may help some women, especially with localized discomfort
Adjust the inputs that commonly worsen flares
Breast tissue can be more reactive during perimenopause. That's why reducing “extra irritation” often helps even when it doesn't eliminate symptoms completely.
A practical starting list:
Lower salt for a few days if swelling is prominent
Reduce caffeine if you notice it tracks with tenderness
Cut back on alcohol if evenings tend to bring more heaviness or heat
Protect sleep because poor sleep amplifies pain sensitivity
Some women keep trying to “push through” breast pain with the same workouts, the same bra, and the same routine. That usually doesn't work. Small mechanical changes often help more than people expect.
Consider body composition and breast weight
After perimenopause, tissue composition shifts can change how the breasts feel and how much pull they create on surrounding structures. Lifestyle changes can significantly impact non-cyclical breast pain linked to weight gain and tissue changes post-perimenopause. As glandular tissue is replaced by fat, increased breast weight can strain ligaments. A 5 to 10% reduction in body fat through targeted exercise has been shown to decrease non-cyclical pain by up to 40% in some women, according to Natural Cycles on perimenopause breast pain.
That doesn't mean every woman with breast pain needs a body-fat goal. It means that if your breasts have become heavier and your pain is more mechanical than cyclical, strength training, posture work, and body-composition changes may be part of what helps.
What often works poorly
A few common approaches tend to disappoint:
Ignoring it for months when the pattern is clearly affecting daily life
Changing five things at once so you can't tell what helped
Assuming every pain is hormonal when posture, medication, or support may be part of it
Wearing a high-impact bra only for workouts but using an unsupportive bra the rest of the day
For supplements such as evening primrose oil, some women report benefit, but results are mixed. I usually suggest treating supplements as optional experiments, not guaranteed solutions, and introducing only one change at a time.
Find Your Pattern by Tracking Your Symptoms
General advice is useful, but it has limits. “Try a better bra” or “cut back on caffeine” only gets you so far if your pain appears randomly, changes quality, or overlaps with poor sleep, stress, and cycle disruption. The most effective move is to stop guessing and start tracking.
While up to 70% of perimenopausal women experience breast pain, most content fails to offer proactive tracking solutions. Emerging AI-powered apps fill this gap by allowing users to log pain intensity and correlate it with cycle phases, diet, and stress, enabling personalized forecasts. Users of such tools often report feeling better within the first week by following a data-informed plan, as described in The Better Menopause guide on sore breasts.
What to track
You don't need a complicated spreadsheet. You need a consistent record.
Track these for a few weeks:
Pain type such as aching, burning, sharp, heavy, swollen
Location in one breast, both, outer side, underarm area, nipple area
Timing morning, evening, around a bleed, after exercise, after poor sleep
Related symptoms including bloating, irritability, hot flashes, headaches
Possible triggers like caffeine, alcohol, stress, bra changes, new workouts
Medication changes especially hormones or antidepressants
Why this changes the conversation
Tracking turns a vague complaint into a usable clinical story. Instead of saying, “My breasts hurt sometimes,” you can say, “This tends to happen three days before bleeding, after poor sleep, and it's worse in the left outer breast when I exercise.” That's far more actionable.
It also helps you identify whether your pain is:
Mostly cyclical
Mostly mechanical
Linked to a medication change
More random than you first thought
If you want a dedicated tool for this, a menopause symptom tracker app can help centralize symptoms, cycle changes, sleep, mood, and daily patterns in one place.
The goal of tracking isn't perfect data. It's pattern recognition.
The hidden benefit
Tracking often lowers anxiety because it replaces the feeling of “this is happening out of nowhere” with “I know what tends to come before this.” That shift matters. It gives you something to work with, something to bring to your doctor, and something to test against your self-care changes.
For painful breasts during perimenopause, pattern recognition is often the difference between feeling ambushed and feeling informed.
When to See Your Doctor and Medical Options
Breast pain is common. It should not be dismissed when the pattern is atypical, persistent, or accompanied by a breast change. The goal isn't to panic. The goal is to know when self-care is enough and when a proper evaluation is the right next step.
When to book an appointment
Noncyclical breast pain can be caused by medications like certain SSRIs and diuretics, or by starting HRT, which causes initial tenderness in 20 to 30% of users. While breast pain is rarely linked to cancer, red flags like a persistent unilateral lump, nipple discharge, or skin dimpling always warrant a medical evaluation to rule out underlying issues like cysts or infections, according to Healthline's review of menopause-related sore breasts.
Make an appointment if you notice:
A lump that persists in the breast or armpit
Pain in one fixed spot that doesn't change or settle
Nipple discharge, especially if spontaneous
Skin dimpling or puckering
Visible breast shape changes that aren't explained by normal cycle shifts
Pain that keeps worsening or interferes with sleep and function
What your clinician may ask
Expect practical questions, not just a quick exam. A good visit usually includes timing, location, what the pain feels like, what medications you take, whether you've started hormone therapy, and whether anything makes it better or worse.
If you're sorting through whether symptoms fit the perimenopause picture more broadly, it can help to compare perimenopause testing options before the appointment so you know what testing can and can't clarify.
You may also find this overview on can you test for perimenopause useful if you're trying to understand where hormone testing fits and where symptom history matters more.
Medical options that may help
Treatment depends on the pattern.
For some women, the plan is simple:
Reassurance after exam and imaging
Medication review, especially if a newer prescription may be contributing
HRT adjustment if tenderness began after starting or changing therapy
Topical pain relief for localized discomfort
For others, the best medical care is clarification, not a prescription. Knowing the pain is benign, hormone-related, or linked to a non-breast source such as chest wall strain can change how you manage it.
Persistent pain deserves an explanation, even when the final answer is “benign.”
Frequently Asked Questions About Perimenopause Breast Pain
Can breast pain come and go during perimenopause
Yes. That's one of the most frustrating parts of it. Pain may flare for a few days, settle, then return at a different point in the month because your cycle is less predictable than it used to be. The quality can change too. One episode may feel like fullness and tenderness, while the next feels sharper or more one-sided.
Does HRT make breast pain better or worse
It can do either. Some women feel more tenderness when they first start hormone therapy because breast tissue is reacting to hormonal input. Others feel better once wider hormone swings calm down. If breast pain starts after beginning HRT, don't guess. Bring the timing to your prescriber and review whether the dose or formulation needs adjusting.
If you're also wondering whether breast pain is one of several signs your hormones are shifting, this overview of 8 key indicators of hormonal imbalance can help you think more broadly about the whole symptom pattern.
Why do breasts still hurt after menopause
When pain continues after menopause, it's less likely to be the classic cyclical pattern and more likely to involve tissue change, breast weight, medication effects, chest wall pain, or a local benign breast issue. Postmenopausal pain also deserves attention because the hormonal explanation becomes less obvious. That doesn't make it dangerous by default, but it does make pattern, location, and associated symptoms more important.
If the pain is new, clearly one-sided, or tied to a lump or visible change, get it assessed.
If you're tired of guessing what your symptoms mean, Lila can help you track breast pain alongside sleep, mood, cycle changes, meals, and other perimenopause symptoms in one place. That kind of daily pattern recognition makes it easier to spot triggers, prepare for flares, and bring clearer information to your doctor.
Get Lila, your personal coach for perimenopause.
Built for women in their 40s. 24/7 coaching, in your pocket.